
Abstract
Introduction and hypothesis
A terminology and standardized classification has yet to be developed for those complications arising directly from the insertion of synthetic (prostheses) and biological (grafts) materials in female pelvic floor surgery.
Methods
This report on the above terminology and classification combines the input of members of the Standardization and Terminology Committees of two International Organizations, the International Urogynecological Association (IUGA) and the International Continence Society (ICS) and a Joint IUGA/ICS Working Group on Complications Terminology, assisted at intervals by many expert external referees. An extensive process of 11 rounds of internal and external review took place with exhaustive examination of each aspect of the terminology and classification. Decision-making was by collective opinion (consensus).
Results
A terminology and classification of complications related directly to the insertion of prostheses and grafts in female pelvic floor surgery has been developed, with the classification based on category (C), time (T) and site (S) classes and divisions, that should encompass all conceivable scenarios for describing insertion complications and healing abnormalities. The CTS code for each complication, involving three (or four) letters and three numerals, is likely to be very suitable for any surgical audit or registry, particularly one that is procedure-specific. Users of the classification have been assisted by case examples, colour charts and online aids (www.icsoffice.org/complication).
Conclusions
A consensus-based terminology and classification report for prosthess and grafts complications in female pelvic floor surgery has been produced, aimed at being a significant aid to clinical practice and research.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Preface
The Standardization and Terminology Committees of the International Urogynecological Association (IUGA) and the International Continence Society (ICS) and the Joint IUGA/ICS Working Group on Complications Terminology seek to provide a terminology and a standardized classification for those complications arising directly from the insertion of prostheses and grafts in female pelvic floor surgery. This document would then be, amongst its various other possible applications such as medical records and surgical audits (often procedure-specific), the basis for a registry of such complications. As the first aim is to standardize the terminology used in this classification, the terms used in the title need to be initially defined.
Classification: A systematic arrangement into classes or groups based on perceived common characteristics [1]. N.B. Division: A separation into two or more parts.
Complication: A morbid process or event that occurs during the course of a surgery that is not an essential part of that surgery (“surgery” replacing “disease” in the definition; “course” includes postoperative of whatever duration) [1].
Directly: Without an intermediary or intervening factor [2].
Related: Connected [2]
Insertion: Putting in [1].
Prosthesis: A fabricated substitute to assist a damaged body part or to augment or stabilize a hypoplastic structure [1].
Mesh: A (prosthetic) network fabric or structure; open spaces or interstices between the strands of the net. [2] The use of this term would be for prolapse surgery with synthetic materials.
Implant: A surgically inserted or embedded prosthesis. [1]. (Explant: a surgically excised prosthesis).
Tape (Sling): A flat strip of synthetic material [1]. The use of this term would be for incontinence surgery with synthetic materials.
Graft: Any tissue or organ for transplantation. [1, 2] This term will be used to refer to biological materials inserted: [3]
-
(a)
Autologous grafts: From patient’s own tissues e.g. dura mater, rectus sheath or fascia lata.
-
(b)
Allografts: From post-mortem tissue banks.
-
(c)
Xenografts: From other species e.g. modified porcine dermis, porcine small intestine and bovine pericardium.
Terminology for grafts has not been separated into the different applications for prolapse and continence surgery.
Trocar: A surgical instrument with either a pyramidal, conical or needle-type cutting or dissecting point.
Introduction
A significant increase in the use of an ever widening array of prostheses and grafts has occurred in female pelvic floor surgery over the last 30 years. In the 1980’s, silastic slings and artificial urinary sphincters [4] were used for urodynamic stress incontinence (USI). McGuire repopularized the rectus sheath fascial sling (an autologous graft) described originally by Aldridge. [5] In the early1990’s, variations on the Stamey-type [6] needle suspension procedures were used involving permanent sutures and modified needles or bone anchors.
In the mid to late 1990’s, suburethral synthetic slings for USI using mesh were introduced, the tension-free vaginal tape (polypropylene mesh) being the most notable. [7] Trocars were used both retropubically and, over the last 8–10 years, laterally passing the obturator membrane and the insertion of the obturator internus muscle. [8] These trocars have the potential for causing trocar insertion-related complications in addition to complications due to the use of the prostheses or grafts themselves.
The prosthetic materials used to date have, in retrospect, been of different surgical propriety, not appreciated at the time of their introduction. Amid [9] has presented a classification for different types of meshes for repair of abdominal wall herniae (the behaviour of meshes around the vagina may differ) based on pore size and fibre type used and the likelihood of complications according to these factors. This has been extremely useful in directing clinicians and the mesh and/or device manufacturers to more appropriate mesh types and designs. The consensus today is that the least morbidity will be achieved by using a low weight, inert, large pore, monofilament prosthesis, with an elasticity between 20% and 35% [10, 11].
Deprest et al [11] have presented an excellent analysis of the biology behind the use of prostheses (synthetic) and grafts (biological) in pelvic organ prolapse repair. The classification to be outlined will cover insertion issues as well as infection, healing abnormalities and other signs of poor integration of these materials, though not the materials themselves.
In terms of prolapse surgery, there has been at times a quest to achieve a prolapse repair with as close to 100% efficacy (anatomical success) and reduce the 29% long-term risk for a woman to undergo a subsequent prolapse surgery after prior prolapse or continence surgery. [12] Anatomical benefits have not been necessarily matched by subjective benefits i.e. functional acceptability for the patient. “Kits” (defined as a set of articles or equipment needed for a specific purpose—[2]) have been introduced for all types of prolapse repairs, again involving the use of different materials with different fixation devices or trocars. Papers on such procedures meeting the scientific criteria for randomized prospective trials have been relatively slow to emerge. In addition to “kits”, the same materials have been also been independently laid in place or fixed with surgical sutures. The use of prostheses or grafts has progressed questionably in some areas from an indication for recurrent prolapse to that of using them in primary procedures. [13]
Historically, discontinuation of a surgical procedure occurs generally due to either (i) a lack of efficacy or (ii) the nature or frequency of complications. Native (patient’s own, not an autologous [transplanted] graft) tissue repairs are also not without complications. Prostheses or grafts potentially add to the complication profile the aspects of (i) trauma of insertion; (ii) reaction of the body to the prosthesis in terms of inflammation or infection; (iii) the stability of the prosthesis over time; (iv) morbidity at the donor site from harvesting an autologous graft.
One key precept in the Hippocratic oath, often quoted in Latin, is primum non nocere (first, to do no harm). Surgeons need to know the possible complications that their surgeries might cause and when and where they might occur. In respect of the use of prostheses and grafts, such information might be generated from a table of complications, (personal, institutional or multi-centre), classified according to three aspects: category, time and site (defined below). In addition, there have been examples of personal, multi-centre, national and industry-coordinated registries. It is a simultaneous aim, with the production of this document, to initiate the development of a user-friendly, online accessible joint ICS-IUGA web-based registry of the complications referred to in this document. With the information from a codified table of procedure-specific complications, possibly involving a registry (at whatever level): (i) a surgeon might better know the value and risk of a certain procedure; (ii) informed counselling might be provided before a woman embarks on that procedure; (iii) if the procedure involves a prosthesis supported by industry, then that group would have detailed feedback on the complications of that procedure. Should the overview in terms of complications be sufficiently adverse, the procedure and/or the prosthesis or graft should be abandoned.
In drawing up such a classification of complications based on category, time and site, the bias would be towards optimising sensitivity, clarity and interpretability. Increasing sensitivity comes with the natural risk of the classification appearing overly complex. It is hoped that the following outline and explanatory notes, user-friendly tables, case examples and some online aids (to be introduced in conjunction with the publication of this document – see abstract and discussion for web reference) might alleviate any such concern. It would be of greater concern if the classification did not cover all the different complication scenarios, such that previously undefined additional terminology might be needed.
Proposed new definitions
Complications involving the use of meshes, tapes and grafts in female pelvic floor surgery need to involve the following viewpoints of (i) local complications; (ii) complications to surrounding organs; (iii) systemic complications. The generic term of “erosion” (medically defined as the “state of being worn away, as by friction or pressure), [1] does not necessarily suit the clinical scenarios encountered. Its use is best avoided, to be replaced by terms with greater physical specificity and clarity.
The additional terms to be used are (see also Table 1):
-
Contraction: Shrinkage or reduction in size [1]
-
Prominence: Parts that protrude beyond the surface [1] (e.g. due to wrinkling or folding with no epithelial separation)
-
Separation: Physically disconnected [2] e.g. vaginal epithelium
-
Exposure: A condition of displaying, revealing, exhibiting or making accessible [1] (e.g. vaginal mesh visualized through separated vaginal epithelium; Fig. 4)
-
Extrusion: Passage gradually out of a body structure or tissue [1]. (e.g. a loop of tape protruding into the vaginal cavity; Fig. 5)
-
Compromise: Bring into danger [2]
-
Perforation: Abnormal opening into a hollow organ or viscus [1]
-
Dehiscence: A bursting open, splitting or gaping along natural or sutured lines [1]
-
Sinus tract formation: (Localized) formation of a fistulous tract towards vagina or skin, where there is no visible implant material in the vaginal lumen or overlying skin.
Category, time and site (CTS) classification
The overall aim of the classification is to summarize any of a large range of possible clinical scenarios into a code (“a numeric system for ordering and classifying information”) [1] using as few as three numerals and three (or four) letters. No additional verbal description, possibly involving undefined terminology, should be necessary (see Table 2).
Selection of categories
The selection of category (C) has used the principal that the least severe complication would involve the prosthesis remaining within the anatomical site into which it was inserted. More severe complications would involve (i) increasing exposure in surrounding anatomical structures; (ii) opening into surrounding organs; and (iii) systemic compromise. The following seven categories (by number) have been formed:
-
1.
Vaginal complication—no epithelial separation: This incorporates the terms prominence (e.g. due to wrinkling or folding) or contraction (shrinkage). Also incorporated here is the palpation of mesh fibres.
-
2.
Vaginal complication—(smaller) exposure: A smaller (1 cm or less) degree of vaginal epithelial separation is involved.
-
3.
Vaginal complication—(larger) exposure or extrusion: A larger degree (more than 1 cm) of vaginal epithelial separation or prosthesis or graft extrusion is involved.
Categories 1–3 have been separated into the following divisions:
-
1A–3A:
Asymptomatic—Abnormal mesh finding These are generally physician-diagnosed at any episode of clinical care. It can be argued that the “abnormal prosthesis or graft finding” aspects of category 1A, in particular, aren’t really complications as the patient isn’t bothered by the potential problem. It may be, however, that the woman may not have engaged in an activity that is likely to provoke symptoms for herself, e.g. pain or bleeding during sexual intercourse (or for her partner), which would convert these complications to category 1B.
-
1Aa–3Aa:
Asymptomatic—Abnormal mesh finding—No pain. The addition of an “a” specifies that the patient experiences no pain in association with the abnormal finding.
-
1Aa–3Aa:
-
1B–3B:
Symptomatic—Unusual discomfort or pain; dyspareunia (for either partner). Bleeding or discharge may be possible symptoms.
-
1Bb–3Bb:
Symptomatic—Provoked pain only (during vaginal examination) The addition of a “b” to the category code specifies that pain, provoked only during vaginal examination, is associated with the abnormal finding.
-
1Bc–3Bc:
Symptomatic—Pain during sexual intercourse The addition of a “c” to the category code specifies that pain, provoked during sexual intercourse (patient only), is associated with the abnormal finding.
-
1Bd–3Bd:
Symptomatic—Pain during physical activities The addition of a “d” to the category code specifies that pain, provoked during physical activities, is associated with the abnormal finding.
-
1Be–3Be:
Symptomatic—Spontaneous pain The addition of an “e” to the category code specifies that pain, spontaneously present (i.e. without physical activity), is associated with the abnormal finding.
-
1Bb–3Bb:
-
1C–3C:
Clinical Infection: This is always a possibility with a synthetic prosthesis or graft. Signs of local tenderness are suggestive with the combination of redness and a purulent discharge being more conclusive.
-
1C–3C (b–e):
Infection—Pain. The addition of the letters “b” through to “e” specifies that pain (as defined in Table 3) is part or all of the infected abnormal finding.
Table 3 Subclassification of Complication Categories to specify the presence of pain (by the patient only, not the partner) associated with the abnormal finding and the grade in terms of the presence and severity of symptoms -
1C–3C (b–e):
-
1D–3D:
Abscess formation: This is a more serious possibility with a synthetic prosthesis or graft.
-
1D–3D (b–e):
Infection—Pain The addition of the letters “b” through to “e” specifies that pain (as defined in Table 3) is part of the abnormal finding associated with abscess formation.
-
1D–3D (b–e):
Category 4: Urinary tract compromise or perforation
This category class has been subdivided into:
-
4A:
Small intraoperative defect: e.g. bladder perforation. Such a complication does not generally create longer-term compromise for the bladder if recognised, prosthesis (graft) removed as indicated, defect oversewn (if necessary), and some minor precautions are taken, e.g. short term bladder drainage, with suitable antibiotics commenced.
-
4B:
Other lower urinary tract (bladder or urethral) complication or compromise: This division would incorporate injuries causing longer term bladder issues, e.g. ongoing prosthesis or graft perforation, fistula, calculus around the prosthesis or graft. This category also incorporates urinary retention directly related to the procedure requiring subsequent surgical intervention (apart from any form of bladder drainage). The time and site divisions relates to those for the surgical intervention.
-
4C:
Ureteric or upper tract complication or compromise:
This division is self-explanatory.
Category 5: Rectal or Bowel compromise or perforation
This category class has been subdivided into:
-
5A:
Small intraoperative defect: Such a complication may not generally be expected to cause compromise if the defect is recognised, prosthesis (graft) removed as indicated, defect oversewn (as necessary) with appropriate precautions taken, e.g. short term bowel rest is instituted with suitable antibiotics commenced.
-
5B:
Rectal injury or compromise: This division would incorporate injuries causing longer term rectal issues, e.g. ongoing prosthesis (graft) perforation, fistula.
-
5C:
Small or large bowel injury or compromise: This division would incorporate injuries causing longer term bowel issues, e.g. ongoing prosthesis (graft) perforation, fistula, obstruction.
-
5D:
Abscess formation from bowel injury/compromise:
Category 6: Skin and/or Musculoskeletal Complications
-
6A:
Asymptomatic: Physician-diagnosed complication at any episode of care.
-
6B:
Symptomatic: e.g. discharge, pain, lump
-
6C:
Infection from skin or musculoskeletal complication: including sinus tract formation
-
6D:
Abscess formation from skin or musculoskeletal complication:
Category 7: Patient compromise
This category recognises that the patient might be brought into systemic danger with some of the complications in addition to any localized issue.
-
7A:
Bleeding complication including haematoma: This division refers to any clinically diagnosed haematoma as well as those where blood transfusion or surgical intervention is a consideration.
-
7B:
Major degree of resuscitation or intensive care: This division refers to significant hemodynamic or cardiopulmonary resuscitation directly related to the procedure, and/or patient transfer for management in intensive care facilities.
-
7C:
Mortality: The insertion of the prosthesis, whilst not necessarily fatal at the time, has set in train further morbid events leading to mortality.
N.B. Because of their systemic nature, 7B and 7C will not have a specific site division. They will be denoted S 0.

Fig. 1 52 year old female underwent a transobturator tape. At 6 weeks, she was cured of her USI and reported no vaginal discharge. Vaginal examination revealed a smaller mesh exposure away from vaginal suture line. Classification:2A T2 S2

Fig. 2. 55 year old female had a retropubic tape. At 2 years follow up, she reported vaginal discharge. Examination revealed a palpable but unseen lateral mesh exposure, together with a cutaneous fistula with local purulent discharge. Classification:(i) 2B T4 S2; (ii) 6C T4 S4

Fig. 3 65-year-old with urinary incontinence, underwent a multifilament transobturator sling. At 14 months follow up, she experienced severe pelvic pain and vaginal discharge. Clinical examination revealed hyperthermia to 40°C, (i) sling exposure at right vaginal sulcus and (ii) severe cellulitis in the genito-crural fold. Classification :3C T4 S2; (ii) 6C T4 S3

Fig. 4. A 67-year-old woman had undergone a vaginal prolapse repair with hysterectomy. She subsequently had a transvaginal mesh repair for a large recurrent cystocele. At 5 months follow up, she complained of dyspareunia. Vaginal examination revealed a mesh exposure of 20 mm by 15 mm at anterior vaginal wall and vaginal cuff. Classification: 3BcT3 S1

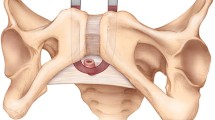
Fig. 5 A 47-year-old woman underwent a transoburator tape for USI. At 5 months follow-up, she reported vaginal discharge. Clinically she was febrile at 38°C with a large sling extrusion as depicted. Classification:3C T3 S1

Fig. 6 A 65-year-old woman underwent a transvaginal mesh repair for a grade 3 prolapse. At 32 months, she had:
-
Recurrent urinary tract infections
-
Urgency and urge incontinence
-
Pelvic pain and deep dyspareunia
-
Bladder pain & lumbar pain
-
Radiology: right hydronephrosis and ureteral obstruction (i)
-
Cystoscopy: mesh extrusion (<0.5 cm) with stone. No right ureteric patency
-
Vaginal examination: (ii) severe anterior mesh shrinkage and pain during anterior vaginal wall palpation. Classification: (i) 4C T4 S3; (ii) 1B c T4 S1
-

Fig. 7 A 56-year-old woman underwent a posterior vaginal mesh procedure using a trocar. At 3 months, clinical examination confirmed an (i) infected midline 15 mm vaginal mesh exposure together with (ii) a recto-vaginal fistula. There had been mesh penetration of the rectum. Classification:3C T3 S1; (ii) 5B T3 S3

Fig. 8 A 62-year-old woman underwent a transobturator anterior vaginal mesh procedure. At 24 months follow up, she reported no vaginal discharge Clinical examination revealed skin erosion with local inflammation and some discomfort at (trocar) exit point. Classification:6B T4 S3
Selection of time (T) divisions
The time (T) for the complication is when it is clinically diagnosed. This section incorporates four time periods, all of the possible episodes where clinical care might be given by the physician or sought by the patient. It might not always be possible to predict with any prosthesis or graft when complications might be more frequently seen. This would depend on the results of a procedure-specific surgical audit using the classification. The earliest time division (T1) might involve more insertion issues, whilst later divisions (T2–T4) might be biased towards healing abnormality issues.
-
T1:
Intraoperative—48 Hours: Insertion complications more likely.
-
T2:
48 hours—2 months: Healing or infection complications more likely.
-
T3:
2 months—12 months: Later healing abnormalities more likely.
-
T4:
Over 12 months: Late healing abnormalities and other mesh complications more likely.
Selection of site (S) divisions
The selection of these divisions incorporates the current sites where prosthesis or graft complications have been noted:
-
S0:
Systemic complications (no specific site): As mentioned earlier, category divisions 7B and 7C which are systemic complications will be denoted S 0
-
S1:
Vaginal: area of suture line: Perhaps the commonest site for prosthesis and graft complications from vaginal surgery is close to the vaginal suture line.
-
S2:
Vaginal: away from the vaginal suture line: As most suture lines would be midline, this would generally be lateral in the vagina.
-
S3:
Trocar passage: The passage of any sharp surgical instrument can cause damage along the path of insertion. This division incorporates any extraperitoneal, bladder or rectal complication, but not intra-abdominal complications which are S5.
-
S4:
Other Skin or musculoskeletal site: This division is relevant to any skin or musculoskeletal complications away from the sites of trocar entry or exit. Included might be cutaneous sinus or fistula formation.
-
S5:
Intra-abdominal: Included in this section would be bowel perforation or obstruction.
CTS Classification: (Complete code):
Example of complete CTS code: 3B/T2/S3 (for simplicity, there is no “C” in front of the category class and division). The letters a to e may be added to the category code e.g. 3Bc/T2/S3 to indicate that pain is part of the abnormality (“c”—pain with intercourse).
Classification guidelines
The following should be noted:
-
Multiple complications may occur in the same patient: These should be reported separately as noted in Table 4.
Table 4 An example of a non-procedure specific table of complications directly related to the insertion of prostheses (meshes, implants, tapes) or grafts in female pelvic floor surgery using the category (C), Time (T) and Site (S) system. The CTS Classification Code is placed adjacent to a description of the complication. One might expect these tables to be often procedure-specific -
There may be early and late complications in the same patient: Again, these should be reported separately.
-
All complications should be listed
-
If there is progression of a particular complication over time, the highest final category is to be used: Progression of a vaginal tape exposure from asymptomatic to symptomatic; an exposure progresses from smaller to larger.
Classification limitations
-
The classification does not note the specific type of mesh: Use of prostheses other than those with the least morbidity (as described in the introduction) might be further reflected in an increased rate of the healing abnormalities.
-
Functional issues (e.g. voiding dysfunction) are not included: Voiding dysfunction can be defined as abnormally slow (assessed by urine flow rate data) and/or incomplete (assessed by postvoid residual) micturition. [14] Surgical intervention for severe voiding dysfunction, namely urinary retention is included in section 4B.
-
Urinary tract infections have not been included.
-
The small risk (about 1 in 2 million) of prion or viral infection associated with a xenograft [15] is not included.
-
Recurrences: It is claimed that meshes are used to prevent recurrence of pelvic organ prolapse. However a mesh procedure might fail resulting in a recurrence. This can be either by degradation or local release of sutures, the clinical result being the same. Sometimes local complications can lead to the removal of the mesh, which could further increase the risk for recurrence. However, it should be emphasized that recurrence is not a complication.
-
Intraperitoneal adhesions: Some procedures involve the use of implant material into the abdomen. As a consequence, intraperitoneal adhesions can arise either on the implant or remotely.
-
Bulking agents: Complications related to bulking agents including migration are not included.
Discussion
The present classification has been developed to be sensitive to all possible physical complications involving the use of a prosthesis or graft in a female pelvic floor surgical procedure. Both insertion complications (e.g trocar related) and healing abnormalities are covered. Whilst this creates a large number of possible complication scenarios, appropriate organization has still been possible by category, time and site. The end-point is a code of 3 letters (4 if “a” to “e” are used) and 3 numerals. The addition of the pain subclassification reflects the recognition of the authors that chronic pain, especially if in the higher subclasses (“c” to “e”), can be amongst the most disabling surgical outcomes from the use of prostheses or grafts in female pelvic floor surgery.
A key advantage of a standardized classification is that all parties involved in female pelvic floor surgery including surgeons, physicians, nurses, allied health professionals and industry will be referring to the same clinical issue. It is anticipated that a (CTS) codified table of complications will be a necessary part of reports of surgical procedures relevant to this document. Many countries already have national data bases for new surgical devices. It is inevitable that there will be more regulation over time for their introduction. With a standardized classification in place, quicker assessment of adverse events will be achieved together with uniform reporting of prosthetic-related complications. Any procedure showing a consistently high rate of complications in a surgical audit would need closer scrutiny and/or possible abandonment. As result of the use of such a classification, in terms of patient care, the principle from the Hippocratic oath, “first, to do no harm” is more likely to be observed.
It is acknowledged that to optimize the coverage of complications, the classification might still appear complex and not immediately mastered. However, as noted in the introduction (page 2), we anticipate that the case examples provided below, the colour charts and the online ICS-IUGA Complication Classification Calculator (www.icsoffice.org/complication) will ameliorate any initial concerns.
It has been a consensus view of the authors that a formal academic terminology and classification should be completed prior to attempts at further simplification. This otherwise might run the risk of compromising coverage of complications.
References
Stedman’s Medical Dictionary (2006) Lippincott, Williams and Wilkins, Baltimore
Concise Oxford Dictionary (1995). Clarendon Press, Oxford
Dwyer PL (2006) Evolution of biological and synthetic grafts in reconstructive pelvic surgery. Int Urogynecol J 17:S10–S15
Duncan HJ, Nurse DE, Mundy AR (1992) Role of the artificial urinary sphincter in the treatment of stress incontinence in women. Br J Urol 69:141–143
Aldridge AH (1942) Transplantation of fascia for relief of urinary stress incontinence. Am J Obstet Gynecol 44:398
Stamey TA (1973) Endoscopic suspension of the vesical neck for urinary incontinence. Surg Gynecol Obstet 136:547–554
Ulmsten UJ, Johnson P, Rezapour M (1999) A three-year follow-up of tension-free vaginal tape for surgical treatment of stress urinary incontinence. Br J Obstet Gynaecol 106:345–350
Delorme E, Droupy S, de Tayrac R, Delmas V (2004) Transobturator tape (Urotape). A new minimally invasive procedure to treat female urinary incontinence. Eur Urol 45:203–207
Amid P (1997) Classification of biomaterials and their relative complications in an abdominal wall hernia surgery. Hernia 1:15–21
Rosch R, Junge K, Hölzl F et al (2004) How to construct a mesh. In: Schumpelick V, Nyhus LM (eds) Meshes: benefits and risks. Springer, Berlin, pp 179–184
Deprest J, Zheng F, Konstantinovic M et al (2006) The biology behind fascial defects and the use of implants in pelvic organ prolapse repair. Int Urogynecol J 17:S16–S25
Olsen AL, Smith VJ, Bergstrom JO et al (1997) Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol 89:501–506
Davila GW (2006) Introduction to the 2005 IUGA Grafts Roundtable. Int Urogynecol J 17:S4–S5
Haylen BT, De Ridder D, Freeman RM, Swift SE, Berghmans B, Lee J, Monga A, Petri E, Rizk DE, Sand PK, Schaer GN (2010). An International Urogynecological Association (IUGA)/ International Continence Society (ICS) joint report on the terminology for pelvic floor dysfunction. Int Urogynecol J 21:5–26 and Neurourol Urodyn 29:4–20
Simonds RJ, Homberg SD, Hurwitz RL (1992) Transmission of human immunodeficiency virus type 1 from seronegative organ tissue donor. N Engl J Med 326:726–730
Acknowledgements
The co-authors acknowledge the support and goodwill of the IUGA and ICS leadership in this second Joint Report from the two societies, following on from the Joint Report on Terminology for Female Pelvic Floor Dysfunction [14]. We thank Mr Dominic Turner and Mr Ashley Brookes from the ICS Office for their assistance and expertise in developing the online aids and the progress towards an ICS-IUGA Registry.
This document has involved 11 rounds of full review by co-authors. Following website publication (Version 8), there have been four rounds of further review. Versions 3 and 10 were subject to live meetings in Cancun (June 2007) and Toronto (August 2010).
The valuable input of Professor Bernard Jacquetin is gratefully acknowledged. The comments of the following reviewers in response to website publication (April to June 2010) are also much appreciated: Dr Angamuthu Arunkalaivanan, Dr Kiran Ashok, Professor Peter Dietz, Dr Nathan Guerette, Professor Don Ostergard and Professor Peter Petros.
Conflicts of interests
BT Haylen: Assistance from Boston Scientific to attend London June 2008 Meeting of the Authors of IUGA-ICS Report on Terminology for Female Pelvic Floor Dysfunction.
RM Freeman: Educational meetings: Astellas and Pfizer. All income from commercial trials and some of the honoraria go to his research fund. Locality lead for the NIHR Peninsula Collaboration for Leadership in Applied Health Research and Care (PenCLAHRC). PROSPECT: A grant holder for this nationally funded trial of prolapse surgery.
SE Swift: No disclosures.
M Cosson: Consultant: Ethicon. Educational sessions: Ethicon, Ipsen. Unconditional grant for fundamental research: Ethicon.
G Willy Davila: Travel expenses or honoraria and consultant: AMS, Novosys. Holds a position of influence in IUGA and NAFC.
J Deprest: Consulting or lecturing: American Medical Systems, Bard, Johnson and Johnson, (Ethicon Gynaecare). His laboratory has received unconditional grants from the same companies, as well as Covidien (formerly Tyco Healthcare).
PL Dwyer: Department research grant from American Medical Systems (AMS).
B Fatton: Consulting or lecturing: Boston Scientific, Astellas and Tena.
E Kocjancic: Consultant: AMS, Coloplast and Bard. Speaker: Astra Zeneca.
J Lee: Travel fellowship awarded by national society; grant sponsored by American Medical Systems.
C Maher: No disclosures.
E Petri: No disclosures.
DE Rizk: No disclosures.
PK Sand: Advisor: Allergan, Astellas, GSK, Coloplast, Ortho, Pfizer, Sanofi, Aventis, Watson. Speaker: Allergan, Astellas, GSK, Ortho, Pfizer, Watson. Investigator: Boston Scientific, Pfizer, Watson, Ortho, Bioform.
GN Schaer: Advisor (in Switzerland): Astellas, Novartis, Pfizer, Gynecare.
R Webb: Travel bursaries: Ethicon, AMS, Pfizer, Astellas. Lecture fees: (departmental) Pfizer, Astellas. Research: Allergan Astellas.
Author information
Authors and Affiliations
Corresponding author
Additional information
International Urogynecology Journal, Vol. 22, No. 1, 2011. Copyright 2011. This material is reproduced with permission of Wiley-Liss, Inc., a subsidiary of John Wiley & Sons, Inc., and the International Urogynecological Association.
This document is being published simultaneously in Neurourology and Urodynamics (NAU) and the International Urogynecology Journal (IUJ), the respective journals of the sponsoring organizations, the International Continence Society (ICS) and the International Urogynecological Association (IUGA) in the January 2011 issue of each journal.
Standardization and Terminology Committee (IUGA) - Bernard T. Haylen, Robert M. Freeman, Steven E. Swift, Peter L. Dwyer, Joseph Lee, Eckhard Petri, Diaa E. Rizk, Peter K. Sand, Gabriel N. Schaer
Standardization and Terminology Committee (ICS) - Robert M. Freeman, Ralph J. Webb
Joint IUGA/ICS Working Group on Complications Terminology - Bernard T. Haylen, Robert M. Freeman, Steven E. Swift, Michel Cosson, Chris Maher, G. Willy Davila, Jan Deprest, Peter L. Dwyer, Brigitte Fatton, Ralph J. Webb
Rights and permissions
About this article
Cite this article
Haylen, B.T., Freeman, R.M., Swift, S.E. et al. An International Urogynecological Association (IUGA) / International Continence Society (ICS) joint terminology and classification of the complications related directly to the insertion of prostheses (meshes, implants, tapes) & grafts in female pelvic floor surgery. Int Urogynecol J 22, 3–15 (2011). https://doi.org/10.1007/s00192-010-1324-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-010-1324-9