
Abstract
Introduction and hypothesis
The current terminology used to describe cosmetic gynecologic procedures includes many nondescriptive, trademarked, or informal names, which contributes to substantial ambiguity about their aims and specific techniques. The development of clear, uniform descriptive terminology for cosmetic gynecology is needed for patients, researchers, and practitioners across multiple specialties.
Methods
This document was developed from a collaboration of selected members from the International Urogynecological Association (IUGA) and the American Urogynecologic Society (AUGS). Wide-ranging literature reviews were performed to identify the breadth of currently used terms and tools for measuring efficacy and safety. After extensive internal review the adoption of each definition was ratified by group consensus.
Results
A terminology report for elective cosmetic gynecology procedures, anatomical classification, outcome metrics, and reporting of complications has been developed. This document seeks to provide clear descriptive guidance for patients, researchers, and practitioners across multiple specialties. This document will be subject to internal review by IUGA and AUGS to incorporate and adopt evidence-based changes in the field.
Conclusions
A consensus-based document establishing clear terminology for cosmetic gynecology procedures has been created. Use of these terms should be encouraged to provide clarity to patients seeking these procedures and to facilitate future research to establish the safety and efficacy of these procedures.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cosmetic gynecology (also known as female genital plastic and cosmetic surgery) lacks standardized nomenclature and procedural definitions. The field is widely understood to encompass an array of interventions to alter the aesthetic appearance of the vulva but is usually also understood to include some elective procedures on the vagina aiming to enhance sexual function. These procedures are typically but not exclusively performed by gynecologists or plastic surgeons, and the terminology used varies by medical specialty and across individual practitioners. The adoption of several colloquial or trademarked phrases (e.g., “O-Shot”), for marketing purposes, has additionally resulted in widespread ambiguity and uncertainty about the aims and actual surgical techniques used in the field.
Most significantly, there is a paucity of high-quality data to support the efficacy and safety of current practice. The American College of Obstetricians and Gynecologists (ACOG) pointedly addressed these concerns in their 2020 Committee Opinion [1] stating that the “safety and effectiveness of these elective procedures have not been well documented.” A previous systematic review [2] has evaluated the existing peer-reviewed literature noting substantial heterogeneity in part due to a lack of standardization of terminology. Despite these concerns, cosmetic procedures are becoming increasingly prevalent [3].
The primary aim of this project was to develop clear, uniform descriptive terminology for cosmetic gynecology that would be useful to patients, researchers, and practitioners across multiple specialties. We aimed to do the following:
-
(1)
Define the clinical domains of Cosmetic Gynecology and distinguish it from (a) medically indicated procedures and (b) female genital mutilation.
-
(2)
Clarify terminology for specific cosmetic gynecology procedures and provide a brief overview of preoperative considerations and therapeutic options.
-
(3)
Suggest clinically meaningful outcome metrics for patients and researchers (when applicable), including collecting or developing standardized classification systems to describe anatomical variants and facilitate uniform reporting of post intervention changes.
-
(4)
Develop a standardized adverse event, reoperation, and revision rate reporting scale tailored to cosmetic gynecology procedures.
This was a joint International Urogynecologic Association (IUGA) and American Urogynecologic Society (AUGS) project consisting of five representative members from each organization and a chair. A literature review of non-medically indicated elective procedures on the labia minora, clitoral hood, labia majora, mons pubis, and vagina was then performed. An iterative discussion then ensued until at least 70% consensus was achieved for each topic.
Consistent with previous IUGA/AUGS Terminology publications this document will not review the clinical evidence or recommend a particular technique. It should be stressed that all procedures considered to be cosmetic are defined in this document irrespective of the presence or absence of peer-reviewed literature. Inclusion of any specific procedure does not constitute an endorsement but rather an objective description for future research. Although this is a developing multidisciplinary field, this document was created by female pelvic medicine & reconstructive surgeons. It does not endorse or make recommendations as to which providers should perform these procedures or what prerequisite experience is required.
Overview of cosmetic gynecology
Definition of cosmetic gynecology
Elective interventions to alter the aesthetic appearance of the external genitalia or modify the genital organs; elective functional vaginal procedures (in the absence of pathology) with the goal of improving a person’s quality of life.
The definition for cosmetic gynecology is intentionally broad to include non-medically indicated procedures performed with the intent to improve a person’s quality of life such as surgical vaginal caliber reduction (vaginal tightening) or injections into the vaginal wall to improve sexual function. These functional procedures have historically been and continue to be considered a facet of cosmetic gynecology.
Although the scope of cosmetic gynecologic procedures appears ambiguous, the main distinction is centered around medical necessity and intent (Fig. 1). A firm distinction must be drawn between surgical intervention predicated upon significant medical pathology such as bothersome pelvic organ prolapse and an elective procedure to improve vaginal laxity in a woman without a diagnosis of a pelvic floor disorder or female sexual dysfunction.

Is this cosmetic gynecology?
Cosmetic gynecology terminology
Much of the ambiguity in cosmetic gynecology stems from the widespread adoption of informal phrases such as “vaginal rejuvenation,” which may be variably interpreted as a labia minora reduction, surgical vaginal tightening procedure, or energy-based treatment. Additionally, the use of trademarked terms compounds the confusion. A hybrid rubric was adopted to balance a call for clear descriptors with the need for simple terms to facilitate discussions with patients (Table 1).
Within the medical community and when describing research, we recommend using the following format: Anatomic Region + Therapeutic Descriptor + Therapeutic Approach. The therapeutic descriptor relays the intended effect such as “augmentation” or “reduction,” whereas the therapeutic approach conveys the utilized technique such as “surgical” or “energy based.”
Therapeutic descriptors
Reduction
Removal of tissue to make smaller or less apparent, generally refers to a surgical excision or lipectomy.
Tightening
To decrease the appearance of loose tissue or feeling of laxity, generally refers to an energy-based approach or any procedure where an area is treated without removal of tissue.
Augmentation
To make larger or change shape/appearance.
Amplification
To enlarge via increase in surface area or functional stimulation effect. Used, for example, to describe elective functional procedures such as clitoral or vaginal injections with the intent of increasing sexual feeling. Different from augmentation, which is purely an anatomic or structural descriptor.
Depigmentation
Decreasing pigmentation in the external genital/perianal skin.
Therapeutic approaches
An in-depth description of operative technique is beyond the scope of this document, which only seeks to define terminology; however, a brief overview is presented.
“Surgical”: The use of scalpel, scissors, electrocautery, and/or sutures to achieve the desired result. Also includes the application of an energy-based medium such as radiofrequency or a laser that would be used in place of a scalpel. Encompasses all manner of procedures not explicitly listed below.
“Energy based”: Application of an energy-based source to the female genitalia with the intent of improving function or aesthetic appearance. A review of these technologies and their potential urogynecologic applications has been published in an AUGS Clinical Consensus Statement [4] and IUGA Committee Opinion [5]. Broadly, energy-based therapies can be divided into lasers (such as carbon dioxide and erbium:yttrium aluminum garnet), radiofrequency, and high-intensity focused ultrasound. The energy source is methodically applied to the target tissue over a single or multiple sessions until the desired effect is achieved.
CO2 lasers were cleared by the FDA in 2010 for “incision, excision, ablation, vaporization and coagulation of body soft tissues in gynecology” and Er:YAG lasers followed in 2014 [6]. Subsequent to this in 2018 the FDA released a Safety Communication warning against the use of energy-based devices for vaginal rejuvenation or vaginal cosmetic procedures citing a lack of safety and efficacy data [7]. Several physician subspecialty organizations have released position statements about the use of laser devices in cosmetic gynecology, warning against use because of a lack of high-quality research [8,9,10].
Lipectomy (liposuction)
The use of cannulas to remove excess undesired adipose tissue. [11].
Filler
Injection of either a biologic or supplementary medium with the intent of either improving aesthetic appearance or (function) enhancing sexual experience. The main categories of filler include:
-
(1)
Platelet-rich plasma (PRP): Whole blood is removed from patient via venipuncture and centrifuged to isolate the platelet-rich portion. This is then activated with calcium to cause platelet degranulation with resultant cytokine and growth factor release, which is then transferred to the target tissue. There is substantial variation in protocol within the literature [12]. PRP consists of various growth factors such as platelet-derived growth factor (PDGF), insulin-like growth factor (IGF), vascular endothelial growth factor (VEGF), and immunologically active agents [13]. The proposed mechanism of action involves the transfer of growth factors and stimulation of cell proliferation. It is FDA approved for use in bone grafts in orthopedic procedures, but has been used off label for androgenic alopecia, cosmetic procedures [12] and repair of vesicovaginal fistulas [14, 15]. It has also been studied with the intent of enhancing sexual responsiveness but there are very few peer-reviewed data to support this [16].
-
(2)
Lipofilling: autologous fat transfer usually via lipectomy of adipose tissue to either enlarge the target tissue or improve aesthetic appearance.
-
(3)
Other biologic fillers including collagen, hyaluronic acid, and amniotic fluid have been utilized for cosmetic indications with minimal supportive data.
It should be noted that fillers are not an approved treatment for female sexual dysfunction (FSD).
Topical ‘T’: Application of a chemical cream or ointment with the intent of improving cosmesis. Some agents that have been utilized for genital depigmentation include lactic acid, azelaic acid, and mandelic acid [17]. The glycolic acid peel (G-Peel) when applied to skin results in desquamation via breakdown of the corneocytes with the overall effect dependent on the concentration of acid and specific technique. This has multiple applications in dermatology including acne, post-inflammatory hyperpigmentation, and photo damage [18]. Recently, it has also been utilized in cosmetic gynecology.
Specific procedures
Labia minora
Anatomy
The labia minora are two skin flaps that originate from the clitoral prepuce and clitoral frenula extending to the posterior fourchette. The labia minora are comprised of non-hair-bearing keratinized squamous epithelium and have minimal connective tissue deeper than the dermis. A systematic review identified significant variation in labia minora length (5–100 mm) and width (1–60 mm) [19]. The largest included study reported measurements of the labia minora in 657 Caucasian asymptomatic women from 15 to 84 years of age with a mean of 43 mm in length (SD 16 mm) and 14 mm in width (SD 7 mm) [20]. Additional research is needed to compare these data to other ethnicities. The labia minora may be hidden beneath or protrude beyond the labia majora with both being considered normal anatomic variants. A cadaveric study showed that the blood supply of the labia minora consists of a dominant central artery, one small anterior artery, and two small posterior arteries [21].
Multiple definitions have been proposed for labia minora hypertrophy with resection potentially indicated at measurements of > 3 [22], 4 [23], or 5 cm [24]. Histologically, hypertrophy describes enlargement of an organ resulting from an increase in the size of its constituent cells. There is evidence to suggest that labia minora enlargement is associated with lymphedema [25], and no study has shown an increase in size of the labia minora cells in women with hypertrophy. In substitution for “hypertrophy,” “labia minora elongation” is a more accurate representation of the clinical assessment of enlarged labia minora. This terminology also has substantial implications as a medical pathology of the labia minora and must be distinguished from a cosmetic preference. Many patients who seek labia minora reduction report both physical and aesthetic indications [26,27,28,29]. As anatomy and reported functional bother are highly variable, a patient-centered definition should be employed.
Labia minora elongation: Any dimension or morphology at which a woman experiences physical discomfort that causes distress and impairs quality of life. Examples include discomfort with exercise or dyspareunia due to enlarged labia minora. This should be considered a medical condition separate from cosmetic gynecology.
Classification
There are numerous systems to classify labia minora anatomy such as the Franco (measures from the introitus to the distal edge) [30], Smarrito (classifying based on location of prominence) [31], or the Motakef (measures on the lateral aspect from the end of the labia majora to the distal edge of the minora; includes annotations for asymmetry or clitoral hood involvement) [32]. An adaptation of these systems is shown in Table 2 with measurement demonstrated in Fig. 2. While labia minora length and location of prominence were not included in this classification, all anatomic factors should be considered prior to intervention.

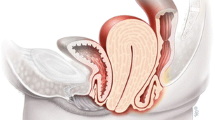
Vulvar anatomy and clitoral/vaginal amplification. (Illustrator: Marie Dauenheimer, MA, CMI, FAMI.)
Examples:
-
(1)
A woman presents with dyspareunia secondary to her labia minora and discomfort during exercise. She does not describe any cosmetic bother and her labia minora measure 6.5 cm (Stage IV-D). This would be considered labia minora elongation as it causes physical symptoms.
-
(2)
A woman with labia minora measuring 5.5 cm reports both physical discomfort and cosmetic bother (Stage III-BD). Although she describes an aesthetic component, she also has symptoms of physical bother so this would also be considered labia minora elongation.
-
(3)
A woman is bothered that her labia minora measuring 5 cm and 3 cm are not symmetric and would like them to be smaller but does not have any physical symptoms (Stage III-AB). This is the only scenario that represents a non-medically indicated cosmetic request.
For research purposes it is helpful to document staging before and after intervention to objectively illustrate the change in anatomy. Photography is also very helpful as all staging systems are limited in descriptive ability.
Procedures
Labia minora reduction-surgical (Fig. 3)
-
(1)
Direct excision: Removal of the distal portion of the labia minora with an energy-based source or scalpel followed by suture closure [33, 34].
-
(2)
Wedge excision: A triangular segment of the labia minora is removed centrally [35] or posterior/laterally [22, 23, 36, 37].
-
(3)
Deepithelialization: Segments of the central epithelium on the medial and lateral aspects of the labia minora are resected and sutured closed with underlying tissue remaining intact [38, 39].
-
(4)
W-Plasty: Intersecting ‘W’ incision lines on the medial and lateral labia minora are resected and joined “valley to peak” [40, 41].
-
(5)
Composite reduction: An extensive direct excision involving superior flaps and a clitoral prepuce reduction described using either RF [42] or CO2 [43].
-
(6)
Z-Plasty: Two ‘Z’ incision lines are made beginning near the base of the central labia minora and fanning out distally. This central segment is resected with the remaining tissue reapproximated [44].
-
(7)
There are multiple variations or combinations of these techniques (e.g., wedge + edge combined resection).

Labia Minora Reduction - Surgical. (Illustrator: Marie Dauenheimer, MA, CMI, FAMI; Original linework by Charlotte Holden.)
Clitoris and clitoral prepuce (hood)
Anatomy
The clitoris is an external organ consisting of a glans, body, root, crura, suspensory ligament, and vestibular bulbs. It is comprised of erectile tissue analogous to the glans penis and may be partially covered by keratinized squamous epithelium in the cephalad area called the clitoral prepuce (clitoral hood). The clitoral frenulum is a fold of tissue on the inferior lateral aspect of the clitoral glans that may join with the anterior labia minora. The measurement of the clitoris in women aged 15–84 years of age varies from 4.62 mm in width and 6.89 mm in length [20]; there are no established normal measurements for the clitoral prepuce. The innervation originates from the bilateral pudendal nerves with the neurovascular bundle running along the superior aspect of the clitoris. The dorsal nerves of the clitoris extend on either side at the 11 and 1 o’clock positions, with the deep dorsal arteries just medial and the paired deep dorsal veins in the center. The superficial dorsal vein courses centrally above the deep dorsal veins [45] (Fig. 2). In an anatomic study of 22 unembalmed female cadavers, the width of the dorsal nerves of the clitoris had a median range of 3 mm at the lateral surface of the crus and 1 mm at the distal body of the clitoris [46]. Knowledge of this anatomy is paramount for anyone performing procedures on the external genitalia.
Clitoromegaly, either congenital or acquired, defined as a clitoral index > 35 mm2 (sagittal diameter mm × transverse diameter mm) [47], is a medical condition, and procedures related to this condition are not considered cosmetic gynecology.
Classification
The labia minora classification system (Table 2) should be used with the ‘C’ annotation for patients who have cosmetic bother of the clitoral prepuce (hood).
Examples:
-
(1)
A woman underwent a labia minora reduction - surgical 6 months ago and now is bothered by excess clitoral prepuce. On examination, her labia minora are symmetric and measure < 2 cm (Stage I-C).
-
a.
Patients interested in a labial reduction surgery should be counseled that, depending on the extent of labia minora removed, it can make the clitoris/clitoral prepuce appear more prominent.
-
b.
Some patients may consider concomitant labia minora and clitoral prepuce procedures.
-
a.
-
(2)
A 37-year-old patient has noticed changes in her labia minora and clitoral prepuce after pregnancy and would like cosmetic intervention. She does not report any physical symptoms. Her labia minora measure 5 cm (Stage III-BC).
-
(3)
A 45-year-old with recent weight gain reports excess clitoral prepuce skin covering the glans clitoris with labia minora that measure 4 cm. After appropriate workup, she does not meet criteria for female sexual dysfunction but desires intervention (Stage II-C).
-
(4)
A woman with a negative screening workup for female sexual dysfunction presents requesting a filler procedure to improve her current sexual function (no classification).
Procedures
Clitoral frenulum reduction-surgical: Surgical removal of a portion of the epithelial folds comprising the frenulum of the clitoris. There is no specific classification for the clitoral frenulum and if performed is commonly paired with labia minora reduction to achieve symmetry.
Clitoral prepuce (hood) reduction-surgical
-
(1)
Lift: A triangular segment of epithelium at the proximal clitoral prepuce (anterior aspect) is resected and reapproximated removing excess tissue.
-
(2)
Parallel ellipses (Fig. 4): Bilateral elliptical spheres of epithelium are resected on either side of the clitoris [34]. This involves vertically oriented elliptical incision in the clitoral hood and linear closure.

Clitoral Prepuce Reduction - Surgical. (Illustrator: Marie Dauenheimer, MA, CMI, FAMI; Original linework by Charlotte Holden.)
A prospective evaluation of women after labia minora reduction and clitoral prepuce reduction found that patients reported either no change or an increase in sensitivity as measured by pressure filament testing at 6 months [34]. Although these results are reassuring given the proximity of the neurovascular bundle to the clitoral prepuce, patients should be counseled extensively about possible loss of sensation in addition to other postoperative complications such as pain, scarring, difficulty with arousal and orgasm, and hypersensitivity [48].
Clitoral amplification-filler
-
(1)
PRP: A topical anesthetic is placed on the clitoris, and venipuncture is performed to obtain PRP, which is then activated with calcium chloride, and 1 ml is injected into the corpus cavernosa of the clitoris (Fig. 2). This may be coupled with injection of 4 ml of PRP into the anterior vaginal wall [49]. As this is a functional intervention there is no classification associated with these procedures. Any patient presenting requesting these procedures should be screened for female sexual dysfunction and referred for appropriate medical treatment as indicated. Filler injections are not evidence-based medical indications for the treatment of female sexual dysfunction.
Labia majora
Anatomy
The labia majora comprise two skin folds extending from the mons pubis toward the perineum, filled with varying degrees of subcutaneous fat. The inner (medial) aspect lacks hair, and the outer (lateral) aspect has hair. The labia majora are separated from the labia minora by a sulcus, which can be absent in some cases, leading to less definition between labia minora and majora. Anatomical variation in the size of the labia majora, including asymmetry, is considered normal [50].
Medical conditions such as genitourinary syndrome of menopause (GSM), formerly known as vulvovaginal atrophy, have been clearly delineated [51]. Aside from a severely atrophic state secondary to a lack of estrogen in postmenopausal women, vulvar dermatologic conditions such as lichen sclerosus, or malignancy, there is no medical pathology associated with the isolated finding of larger or smaller labia majora.
Classification
Fasola and colleagues have proposed one classification system wherein they divided labia majora hypotrophy in three stages based on the appearance of subcutaneous layers, cutaneous layers, and symptoms [52]; however, this system incorporates medical pathologies such as GSM. There are other prior descriptions of labia majora hypertrophy or labia majora hypotrophy; however, this terminology implies that an anatomical norm exists. In substitution for these phrases, patients may be described as either “desiring reduction” or “desiring augmentation” without labeling anatomy as abnormal (Table 3).
Examples:
-
(1)
A 70-year-old female with complaints of dryness and pruritis of the external genitalia confirmed on examination without request for cosmetic alteration (Stage 0). This patient has physical symptoms and should be evaluated for medical pathology.
-
(2)
A woman reports asymmetric labia majora and would like a surgical reduction (Stage II-A).
-
(3)
A 45-year-old female who presents after massive weight loss from a combination of lifestyle modification and bariatric surgery who desires removal of excess skin on her labia majora (Stage II-L).
-
(4)
A 53-year-old female without physical symptoms or bother requests filler injections into the labia majora as she has noted decreased volume and some laxity over recent years (Stage I-L).
In the above examples, patients presenting with complaints of labia majora skin laxity may potentially request either an augmentation or reduction with either option being therapeutic.
Procedures
Labia majora reduction procedures
Performed with the goal of reducing the dimensions or prominence of the majora (Fig. 5).

Labia majora modification. (Illustrator: Marie Dauenheimer, MA, CMI, FAMI.)
Labia majora reduction-surgical
An elliptical or bow-shaped incision is made on the inner aspect of the labia majora to remove excess epithelium and adipose tissue (if desired).
Labia majora reduction-lipectomy
Liposuction of the labia majora. This may be performed concomitantly with a mons pubis procedure to address excess tissue after massive weightloss [53]. Isolated lipectomy of this area may result in skin laxity ‘L’, so patients electing this procedure should be counseled to determine whether removal of redundant epithelium is desired.
Labia majora tightening-energy based
Treatment of the labia majora with radiofrequency, CO2, or erbium:Yag laser with the intent of firming or tightening the skin. Radiofrequency [54,55,56,57,58,59] and Er:YAG lasers [60, 61] have been evaluated for the treatment of vaginal and/or vulvar laxity.
Patients should be counseled that reduction of the labia majora could potentially make the labia minora appear larger or more prominent.
Labia majora augmentation procedures
Performed with the goal of increasing the volume and hydration of the labia majora.
Labia majora augmentation-filler
-
(1)
Lipofilling: An autologous fat graft is injected in layers into the labia majora [62,63,64].
-
(2)
Hyaluronic acid filling: Variable volumes of hyaluronic acid are injected into the subcutaneous tissue [52, 65].
Labia majora augmentation-surgical:
-
(1)
Adipofascial flap: performed concurrently with a thigh lift using a de-epithelialized adipofascial flap raised from the inner thigh [66].
-
(2)
Labia minora transposition: involves de-epithelializing the protruding part of the labia minora and transposing this into a pocket created in the labia majora [67].
-
(3)
Dermal graft: inserting two de-epithelialized dermal fat grafts into tunnels created bluntly on the medial aspect of the labia majora [68].
A systematic review assessing techniques and outcomes of cosmetic labia majora augmentation has been published [69].
Mons pubis
Anatomy
The mons pubis or mons veneris refers to the rounded region and fat pad overlying the pubic symphysis [70]. The mons has vague anatomic boundaries roughly defined as the top of the hair-bearing pubic area, the inguinal crease laterally, and the anterior labial commissure inferiorly. It is generally convex with an outward bulge created by a superficial fatty deposit that thins at the anterior labial commissure and is separated by the superficial fascial system, which continues as Colles’ fascia containing the deeper adipose tissue layer into the labia majora.
Indications
Overgrowth or excessive size has been termed hypertrophy and may be associated with laxity and/or ptosis. Weight changes (particularly weight loss), pregnancy, and familial fat distribution can cause the appearance of ptosis, laxity, contour deformities, redundancy, and overlapping skin roll [71]. These changes may be associated with psychosocial distress, impaired quality of life, poor hygiene, difficulty dressing, limit movement, and urinary or sexual dysfunction.
Mons pubis ptosis
The visual appearance of an overhang or drooping of the adipose tissue of the mons pubis.
Classification
There are two widely used classification systems for the mons pubis: the Pittsburgh Rating Scale [72] and the El-Khatib Grading System are well described in the plastic surgery literature [73].
-
(1)
The Pittsburgh Rating scale [72] is designed to evaluate regional body deformities in patients after massive weight loss and for postoperative evaluation. A 3-point subsection is included to assess the mons pubis.
-
a.
Score 0: No visible abnormality and no intervention.
-
b.
Score 1: Excessive adiposity with recommendation for ultrasound assisted lipectomy (UAL) or suction assisted lipectomy (SAL).
-
c.
Score 2: Ptosis: Recommendation for monsplasty
-
d.
Score 3: Significant overhang below symphysis, recommendation for monsplasty.
-
a.
-
(2)
El-Khatib et al.'s system [73] of mons pubis deformity and strategy recommendation for treatment is graded on a 4-point scale.
-
a.
Grade 1: mild bulging with minimal or no covering external genitalia and a recommendation for liposuction alone.
-
b.
Grade 2: moderate bulging with partial covering of external genitalia, recommended for liposuction-assisted panniculectomy.
-
c.
Grade 3: bulging with complete covering of external genitalia, recommended for liposuction assisted panniculectomy and fascial dermal suspension with or without vertical wedge excision for horizontal laxity.
-
d.
Grade 4: No bulging with partial or complete covering external genitalia, recommendations the same as grade 3 with addition of vertical wedge excision.
-
a.
Most cosmetic mons pubis procedures are performed by plastic surgeons, and the classification schemes above are objective, well defined, and include treatment options.
Procedures
The primary aim is to create a smooth transition from the lower abdomen to the vulva (Fig. 6).

Mons pubis modification. (Illustrator: Marie Dauenheimer, MA, CMI, FAMI.)
Mons pubis reduction-surgical
Excessive skin and fat are removed by dissecting to the level of the mons pubis fascia along an area bordered superiorly at abdominoplasty or prior scar and inferiorly approximately 5–7 cm above the anterior vulvar commissure. Lateral incision shapes can vary by technique including trapezoidal shape [74, 75], circular arch [53, 76], swallow crescent [53], sharp triangular wedge [73, 77], and continuous abdominoplasty incisions extending laterally over upper thighs corresponding to parallel abdominoplasty incision [77]. The mons pubis is then anchored to the abdominal fascia with permanent or delayed absorbable sutures [53, 73,74,75, 77].
This procedure is commonly performed with an abdominoplasty or panniculectomy. If the mons pubis is not addressed at the time of abdominal contouring the patient may be left with an unsatisfactory aesthetic result. Additionally, performing a surgical mons pubis reduction at the time of a labia minora reduction procedure could lead to overcorrection and painful tightening of the pubic region [53, 74].
Mons pubis tightening-energy based
Treatments using radiofrequency technology to reduce ptosis and tighten the region [78, 79]. This will have a more modest effect relative to surgical intervention or lipectomy.
Mons pubis reduction-lipectomy
Liposuction of the mons pubis.
-
(1)
Suction-assisted lipectomy (SAL): technique involving suction aspiration of adipose tissue through a cannula.
-
(2)
Ultrasound-assisted lipectomy (UAL): utilizing high-frequency ultrasonic waves either externally or internally to liquify adipocytes prior to removal with a suction cannula device.
Reported risks of mons pubis reduction/lipectomy include prolonged edema, lymphedema, hematoma, and loss of sensation in the region [71, 76, 80].
Vagina
Anatomy
The vagina is a tubular structure that extends from the uterine cervix proximally and attaches to the vulva distally. The vaginal wall consists of the epithelium, lamina propria, muscularis, and areolar connective tissue. Vaginal support has been described as proximal support (Level I), mid-vaginal/lateral support (Level 2), and distal/perineal body support (Level 3) [81].
The distal aspect of the anterior vaginal wall has been both a therapeutic target and area of controversy since the area was first described by Grafenberg in 1950 and later referred to as the “G-spot” in 1981 by Addiego. It has been suggested that stimulation of this area can result in arousal, orgasm, and female ejaculation. Much of the evidence to support these claims is anecdotal if not questionable [82]. Although histologic studies have yielded conflicting results, recent work suggests that neurovascular structures along the anterior vaginal wall have a uniform distribution as opposed to concentration in one small area [83]. Nevertheless, health care providers have sought to amplify the G-spot via various types of filler to improve sexual function [84].
Vaginal laxity is a symptom that has broad associations including being a symptom of prolapse and a complaint of excessive vaginal looseness [85,86,87]. Women with vaginal laxity may experience sexual dysfunction that manifests as a dyspareunia, increased vaginal ‘wind,’ obstructed intercourse, or loss of or decreased libido [85, 88]. They may also describe entrapment of bath or shower water in the vagina, which empties upon standing or difficulty retaining a tampon. Among 324 urogynecology patients, vaginal laxity was reported by 24% with a mean bother of 5.7 (on a 0–10 Likert scale) [87]. Vaginal laxity was associated with younger age, vaginal parity, prolapse symptoms and bother, objective prolapse, and wider genital hiatus on Valsalva maneuver, which suggests vaginal laxity may be a manifestation of levator ani hyperdistensibility. Campbell and colleagues [89] noted that vaginal laxity was reported by 38% of 22,621 women attending the urogynecology clinic, and was associated with vaginal parity, prolapse symptoms, stress and urge urinary incontinence, reduced sexual sensation, and worse general life as reported on the Personal Assessment Questionnaire-Pelvic Floor (ePAQ-PF). However, the report of vaginal laxity may also be due to male sexual dysfunction. In a IUGA survey of physician members 83% of respondents felt that vaginal laxity was underreported by patients [90].
Classification
Objective evaluation of vaginal laxity has not been standardized, but a variety of measurements have been proposed. Haylen and colleagues [85] describe the following measurements:
-
(1)
Perineal gap: the distance (in cm) between forceps placed bilaterally where the labia minora meet the perineum.
-
(2)
Mid-vaginal laxity: the laxity of the mid-posterior vaginal epithelium with vaginal apical traction.
-
(3)
Recto-vaginal fascial laxity: the laxity of the mid-vaginal rectovaginal fascia once the epithelium is incised and the vaginal apex is supported.
During evaluation clinically significant pelvic organ prolapse or female sexual dysfunction should be ruled out as this would constitute a medical pathology. The Pelvic Organ Quantification (POP-Q) system is widely adopted and very descriptive in objectively reporting vaginal anatomy. The annotation of vaginal laxity should only be utilized if the patient reports this symptom as bothersome (Table 4).
Examples:
-
(1)
A 32-year-old P3 with a history of a prior forceps delivery presents describing a feeling of decreased friction and vaginal laxity during intercourse. She does not have significant pelvic organ prolapse (Point Ba-2, Bp-2, C-7); however, her genital hiatus is 4.5 (Stage IL).
-
(2)
A 67-year-old P4 with a prior hysterectomy who is not sexually active reports a persistent vaginal bulge (Point C +3, Aa +1, Ba +1) with a genital hiatus of 5 (Stage III-C, as patient does not report any vaginal laxity). She has medically significant POP, and there is no associated cosmetic indication. Although her genital hiatus is enlarged at 5 cm, the perception of vaginal laxity is not bothersome to her (but the pelvic organ prolapse and symptoms of bulging and pressure are), so no additional ‘L’ annotation is included in her staging.
Procedures
Vaginal reduction-surgical: procedure with the intent of narrowing the either the entire vaginal caliber or the genital hiatus.
-
(1)
Posterior vaginal repair, levator plication, and perineal repair: These procedures are described in detail in an AUGS/IUGA Terminology Report on Surgical Procedures to Treat Pelvic Organ Prolapse [91].
-
(2)
Perineal repair: An isolated perineal repair as described [91] can be performed on patients without vaginal laxity who only desire an alteration in the appearance of the genital hiatus.
-
(3)
Lateral colporrhaphy: An isolated excision of bilateral ellipses of vaginal epithelium on the posterior lateral wall has been described [92].
Vaginal tightening: energy based
Treatment of the vagina with radiofrequency, CO2, or ER:Yag laser with the intent of firming or tightening the vaginal caliber. Radiofrequency [54,55,56,57,58,59] and Er:YAG lasers [60, 61] have been evaluated for the treatment of vaginal and/or vulvar laxity. High intensity focused ultrasound (HIFU) and carboxy therapy have been described and are promoted for vaginal tightening and vulvar stretch marks; however, no published research is available at this time to justify these treatments.
Vaginal amplification-fillers:
-
(1)
Platelet-rich plasma: injection of platelet-rich plasma into the anterior vaginal wall with the intent of increasing the size and sensitivity of the area (G-spot). These procedures have been marketed as treatments for female sexual dysfunction, decreased libido, or orgasmic dysfunction; however, it should be clearly stated that these are medical conditions and there is not good evidence to support injection of fillers as a treatment for these conditions.
-
(2)
Hyaluronic acid gel: Injected into the distal anterior vaginal wall with the aim of increasing contact of this area during intercourse. Severe pulmonary complications and two deaths have been reported after hyaluronic injection into the vaginal wall [93,94,95].
-
(3)
Autologous fat transfer: 8 cc autologous fat graft injected into the anterior vaginal wall 5 cm away from the introitus [96].
Although this document only seeks to describe reported procedures without discussion of the available evidence, it should be clearly stated that there are very minimal published peer reviewed data on the injection of fillers in the anterior vaginal wall [97].
Genital depigmentation
This topic is listed separately as it may include the vulvar structures, perineum, and/or anus. Some patients request cosmetic procedures with the goal to achieve pigmentation that is consistent with the skin color of surrounding areas (e.g., skin of the buttocks). If multiple areas are treated, it should be described as “anogenital;” otherwise, individual anatomic regions (e.g., “anal” or “vulvar”) should be used.
Hyperpigmentation may occur as a result of irritation from shaving or waxing [98] or other factors such as pregnancy, medical conditions, or medications. Patients should be cautioned that there are few if any peer-reviewed safety and efficacy data on this topic, prior to undergoing treatment.
Procedures
Genital depigmentation-energy based: utilized to treat areas of hyperpigmentation.
-
(1)
Fractional CO2 laser
-
(2)
Picosecond laser
-
(3)
Radiofrequency: Although not directly resulting in decreased pigmentation after treatment, the tissue may lighten.
Genital depigmentation- topical:
-
(1)
Chemical Peel: Mixtures of phytic, retinoic, and azelaic acid are applied to the genitalia removing the external skin resulting in smoother, lighter appearance [17].
-
(2)
Glycolic acid peel: Glycolic acid solution is applied to the genitalia for 20 min and removed with water. This process is repeated every 15 days for eight total treatments [17].
-
(3)
Application of individual agents such as lactic acid, azelaic acid, or mandelic acid.
Outcome metrics
Demonstration of efficacy is challenging in cosmetic gynecology as both aesthetics and the perception of vulvar or vaginal laxity are subjective. A systematic review of patient-reported outcome measures identified 50 questionnaires of which 26 were ad hoc metrics and 22 were generic surveys with only two validated instruments specific for cosmetic gynecology [99]. Although ideal aesthetic proportions or ratios have been proposed in the literature for the face, lips, and body, this should be avoided for cosmetic gynecology. The patient should be counseled that her anatomy is normal and there is no “ideal” size or shape of the female genitalia. We recommend a focus on patient-centered outcomes.
Labia minora outcomes
The Genital Appearance Satisfaction Scale (GAS) [100] is a validated 11-item questionnaire designed and developed as a research tool to assess vulvar and vaginal perception in the general population and was later applied to patients seeking labiaplasty [101, 102]. Subjects are asked to rate eight negative and three positive statements about genital appearance on a 0–3 scale (Supplement A). The Cosmetic Procedures Scale- Labia (COPS-L), validated as a screening tool for body dysmorphic disorder [101], has also been utilized to evaluate outcomes after intervention [102].
Vaginal and vulvar laxity outcomes
There are no validated measures for vaginal or vulvar laxity. Some research studies utilize proxy measures such as the Female Sexual Function Index (FSFI) [103] or Female Sexual Distress Scale (FSDS); however, these metrics are neither specific for nor focused on detecting changes in laxity. The Vaginal Laxity Questionnaire (VLQ) [55] is a 7-point Likert scale, ranging from “very loose” to “very tight,” that has been frequently used to assess efficacy [54,55,56,57] (Supplement B). Utilization of the Brink’s score and perineometry [61], which measure pelvic floor muscular tone and strength, have been reported as end points; however, this is unlikely correlated with improvement of vaginal laxity. In assessing vulvar laxity, the use of photography pre- and post-treatment is crucial, as there are no objective metrics that can be employed. For research purposes, the use of blinded evaluators [58, 59] assessing results is crucial to minimize bias.
Classification of Complications and Revisions
Widespread reporting of a standardized adverse event scale is crucial in the determination of safety profiles. The Clavien-Dindo Complication Scale [104] was adapted for cosmetic procedures (Table 5). Specifically, there is a need to distinguish categories of repeat intervention for patient satisfaction versus surgical complication.
Revision rate: Surgical revision for an aesthetic indication. For example, if a patient undergoes a labia minora reduction-surgical and postoperatively is not satisfied because of a perceived under-correction (inadequate reduction), this would be classified as a “Grade 0-u.” Although not technically a medical complication, this is a suboptimal outcome and as such it should be reported.
Reoperation rate: Requiring surgical intervention for a medical complication. In a scenario where a suboptimal aesthetic outcome is coupled with a medical complication requiring intervention, only a “Grade III” complication should be reported.
Preoperative counseling
Common motivating factors for women undergoing cosmetic gynecology procedures may include appearance, function, sexuality, or psychologic factors. As with all surgical interventions, extensive preoperative counseling is paramount. In addition to obtaining a baseline history, particular emphasis should be placed on age, social functioning, relationships, quality of life, personality profile, previous cosmetic surgery, functional symptoms, aesthetic symptoms, comorbidities, and expectations.
Surgeons must ensure that patients understand the implication of possible adverse events and that they may not be satisfied with the operative result. Written documentation of patients’ preferences and information about the surgical procedure/aim should be outlined in a very detailed manner and accompanied by photo documentation whenever possible. Cosmetic gynecology procedures on individuals < 18 years of age are contraindicated.
For all anatomic regions in this document, reassurance about variations in individual anatomy is always appropriate, and intervention is never mandatory if the concern is purely cosmetic.
Body dysmorphic disorder
Body dysmorphic disorder (BDD) is a psychiatric disorder characterized by significant distress caused by a minor physical defect. People with BDD often elect cosmetic surgery to have the alleged defects corrected [105, 106]. In the US, 7–8% of patients undergoing plastic surgery have BDD with a range of 3–53% in international studies [107,108,109,110,111,112]. There is no evidence that there is an improvement in the level of suffering after a cosmetic operation in women with BDD and that surgery should therefore be refused in these cases [113]. Therefore, all patients pursuing cosmetic gynecologic surgery should be screened for body dysmorphic disorder with a questionnaire such as the Body Dysmorphic Disorder Questionnaire (BDDQ) [114] or the Cosmetic Procedure Screening Scale (COPS) [115]. The COPS-L is a modification of the COPS survey that has been validated in women seeking labiaplasty with scores > 45 requiring further assessment for BDD [101]. Practitioners should have a low threshold for referral to a mental health professional if there is any suspicion of BDD or underlying psychiatric diagnosis.
Ethical principles and procedures not included
It is also imperative that motivators are clear and patients are free from coercion from any outside influence (including health care providers). The ethics surrounding cosmetic gynecology has been discussed in previous editorials [116,117,118]. As these procedures are generally on a fee-for-service or cash-based model, there is potential for physician conflict of interest. To further clarify, a brief discussion of ethical principles is warranted (Table 6).
In applying these ethical principles, the scope of cosmetic gynecology may be further defined through a description of excluded topics: female genital mutilation and surgical reconstruction of the hymen.
Female genital mutilation
Female genital mutilation (FGM): The World Health Organization (WHO) defines FGM as “all procedures that involve partial or total removal of the female genitalia and/or injury to the female genital organs for cultural or any other non-therapeutic reasons” [119]. FGM is stratified into four distinct types (Supplement C) [119] and is generally performed on young girls between infancy and 15 years of age by either a traditional circumciser or by a health care professional (who offers this with the belief that it will be safer when medicalized) [120].
FGM is defined very broadly by the WHO to encompass any nonmedical alteration of the female genitalia. A sharp distinction should be made between these FGM practices, which in many instances are performed either against a woman’s will or with the intent to cause physical or psychologic harm versus cosmetic gynecology procedures which are patient-driven elective procedures to address a cosmetic or nonmedical functional concern specifically requested by a consenting adult under her own volition. FGM is a very complex topic with social and cultural implications, and a complete discussion is beyond the scope of this document; however, it is presented here to distinguish it from cosmetic gynecology. Please refer to the World Health Organization (WHO) for further guidance on this topic.
Surgical reconstruction of the hymen
The hymen is a membranous vestige of the junction between the sinovaginal bulb and the urogenital sinus. Congenital anomalies such as imperforate, microperforate, or septate hymen are medical pathologies warranting appropriate workup and intervention as necessary [121]. Reconstruction of an anatomically normal hymen has been described in the literature but is not considered cosmetic gynecology because of ethical concerns. Surgical intent may vary but many patients seek this procedure as a “certificate of virginity” [122]. This can include visual integrity or a desired goal of bleeding with penetrative intercourse. In some cultures, a woman who is determined to not be a virgin on her wedding night can be harmed or killed [123].
Patients requesting procedures on the hymen should be counseled that these interventions have no direct medical benefits [124], and complications may include bleeding, infection, or dyspareunia. Absence of an intact hymen or failure to bleed upon penetration is not a sign of previous intercourse. Only 34% of virginal females reported blood loss during their first sexual encounter [125]. Each request for hymenoplasty should be taken with care to address any underlying concerns through education of the patient, partner, and family members.
Hymenoplasty, surgical reconstruction of the hymenal ring (Supplement D) [123, 126,127,128,129], is not considered a cosmetic procedure.
Conclusion
This IUGA/AUGS joint working group recognizes that there is substantial ambiguity concerning the terminology, classification, adverse event reporting, and outcome metrics in the field of cosmetic gynecology. We also acknowledge that these procedures are being offered on a fee for service basis across the world and that the efficacy of many of these techniques has not been fully investigated. Without either endorsing or denouncing any of topics within cosmetic gynecology, this document seeks to establish a framework and uniform language upon which future research can be conducted in an effort to improve safety, advance evidence-based medicine, and empower women. Most importantly, it should be re-emphasized that all anatomic variants, unless they cause physical discomfort or bothersome symptoms, are normal.
References
ACOG. Committee opinion #795: elective female genital cosmetic surgery. Obstet Gynecol. 2020;135(1):e36–42.
Garcia B, Scheib S, Hallner B, Thompson N, Schiavo J, Peacock L. Cosmetic gynecology — a systematic review and call for standardized outcome measures. Int Urogynecol J. 2020;31(10):1979–95.
Liao LM, Creighton SM. Requests for cosmetic genitoplasty: how should healthcare providers respond? Bmj. 2007;334(7603):1090–2. https://doi.org/10.1136/bmj.39206.422269.be.
Alshiek J, Garcia B, Minassian VA, et al. Vaginal energy based devices – AUGS clinical consensus statement. Female Pelvic Med Reconstr Surg. 2020;26(5):287–98. https://doi.org/10.1097/SPV.0000000000000872.
Shobeiri SA, Kerkhof MH, Minassian VA, Bazi T. IUGA committee opinion: laser-based vaginal devices for treatment of stress urinary incontinence, genitourinary syndrome of menopause, and vaginal laxity. Int Urogynecol J. 2019;30:371–6.
Tadir Y, Gaspar A, Lev-Sagie A, et al. Light and energy based therapeutics for genitourinary syndrome of menopause: consensus and controversies. Lasers Surg Med. 2017;49(2):137–59. https://doi.org/10.1002/lsm.22637.
Safety Communications - FDA Warns Against Use of Energy-Based Devices to Perform Vaginal BRejuvenation^ or Vaginal Cosmetic Procedures: FDA Safety Communication. https://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm615013.htm. Accessed Aug 15 2018.
FDA Mandating Vaginal Laser Manufacturers Present Valid Data Before Marketing; 2018.
Shobeiri SA, Kerkhof MH, Minassian VA, Bazi T. IUGA committee opinion: laser-based vaginal devices for treatment of stress urinary incontinence, genitourinary syndrome of menopause, and vaginal laxity. Int Urogynecol J. 2019;30(3):371–6. https://doi.org/10.1007/s00192-018-3830-0.
Preti M, Vieira-Baptista P, Digesu GA, et al. The clinical role of LASER for vulvar and vaginal treatments in gynecology and female urology: an ICS/ISSVD best practice consensus document. Neurourol Urodyn. 2019;38(3):1009–23. https://doi.org/10.1002/nau.23931.
Chia CT, Neinstein RM, Theodorou SJ. Evidence-based medicine: liposuction. Plast Reconstr Surg. 2017;139(1):267e–74e. https://doi.org/10.1097/PRS.0000000000002859.
Kramer MJE, Keaney TC. Systematic review of platelet-rich plasma (PRP) preparation and composition for the treatment of androgenetic alopecia. J Cosmet Dermatol. 2018;17(5):666–71. https://doi.org/10.1111/jocd.12679.
Xie X, Zhang C, Tuan RS. Biology of platelet-rich plasma and its clinical application in cartilage repair. Arthritis Res Ther. 2014;16(1):1–15. https://doi.org/10.1186/ar4493.
Streit-Ciećkiewicz D, Futyma K, Miotła P, Grzybowska ME, Rechberger T. Platelet-rich plasma as adjuvant therapy for recurrent Vesicovaginal fistula: A prospective case series. J Clin Med. 2019;8(12):2122. https://doi.org/10.3390/jcm8122122.
Streit-Ciećkiewicz D, Nowakowski Ł, Grzybowska ME, Futyma K. Predictive value of classification systems and single fistula-related factors in surgical management of vesicovaginal fistula. Neurourol Urodyn. 2021;40(1):529–37. https://doi.org/10.1002/nau.24594.
Runels C, Melnick H, Debourbon E, Roy L. A pilot study of the effect of localized injections of autologous platelet rich plasma (PRP) for the treatment of female sexual dysfunction. Int Open Access J Women’s Heal Care. 2014;3(4):1–4. https://doi.org/10.4172/2167-0420.1000169.
Hamori C, Banwell P, Alinsod R, eds. Female Genital Cosmetic Surgery Concepts, Classifications, & Techniques. Thieme; 2017.
Sharad J. Glycolic acid peel therapy - A current review. Clin Cosmet Investig Dermatol. 2013;6:281–8. https://doi.org/10.2147/CCID.S34029.
Hayes JA, Temple-Smith MJ. What is the anatomical basis of labiaplasty? A review of normative datasets for female genital anatomy. Aust New Zeal J Obstet Gynaecol. 2020:1–8. https://doi.org/10.1111/ajo.13298.
Kreklau A, Vâz I, Oehme F, et al. Measurements of a ‘normal vulva’ in women aged 15–84: a cross-sectional prospective single-Centre study. BJOG An Int J Obstet Gynaecol. 2018;125(13):1656–61. https://doi.org/10.1111/1471-0528.15387.
Georgiou CA, Benatar M, Dumas P, et al. A cadaveric study of the arterial blood supply of the Labia minora. Plast Reconstr Surg. 2015;136(1):167–78. https://doi.org/10.1097/PRS.0000000000001394.
Munhoz AM, Filassi JR, Ricci MD, et al. Aesthetic labia minora reduction with inferior wedge resection and superior pedicle flap reconstruction. Plast Reconstr Surg. 2006;118(5):1237–47 https://doi.org/10.1097/01.prs.0000237003.24294.04.
Rouzier R, Louis-Sylvestre C, Paniel BJ, Haddad B. Hypertrophy of labia minora: experience with 163 reductions. Am J Obstet Gynecol. 2000;182(1 Pt 1):35–40.
Ellsworth WA, Rizvi M, Lypka M, et al. Techniques for labia minora reduction: an algorithmic approach. Aesthet Plast Surg. 2010;34(1):105–10. https://doi.org/10.1007/s00266-009-9454-5.
Barrett MM, Carlson JA. A clinicopathologic study of labia minora hypertrophy: signs of localized lymphedema were universal. J Low Genit Tract Dis. 2014;18(1):13–20. https://doi.org/10.1097/LGT.0b013e31828d3989.
Miklos JR, Moore RD. Labiaplasty of the labia minora: patients’ indications for pursuing surgery. J Sex Med. 2008;5(6):1492–5. https://doi.org/10.1111/j.1743-6109.2008.00813.x.
Goodman MP, Placik OJ, Benson RH 3rd, et al. A large multicenter outcome study of female genital plastic surgery. J Sex Med. 2010;7(4 Pt 1):1565–77. https://doi.org/10.1111/j.1743-6109.2009.01573.x.
Pardo SJ, Solá DV, Galán CG, Contreras ML. Labioplastía genital, experiencia y resultados en 500 casos consecutivos. Rev Chil Obstet Ginecol. 2015;80(5):394–400. https://doi.org/10.4067/s0717-75262015000500007.
Propst K, Ferrando CA. Outcomes of labiaplasty in women with labial hypertrophy. Int Urogynecol J. 2021;32:1247–51. https://doi.org/10.1007/s00192-020-04621-w.
Franco T, Franco D. Hipertrofia de Ninfas. J Bras Ginecol. 1993:163–5.
Smarrito S. Classification of labia minora hypertrophy: A retrospective study of 100 patient cases. JPRAS Open. 2017;13:81–91. https://doi.org/10.1016/j.jpra.2017.05.013.
Motakef S, Rodriguez-Feliz J, Chung MT, Ingargiola MJ, Wong VW, Patel A. Vaginal labiaplasty: current practices and a simplified classification system for labial protrusion. Plast Reconstr Surg. 2015;135(3):774–88. https://doi.org/10.1097/PRS.0000000000001000.
Pardo J, Sola V, Ricci P, Guilloff E. Laser labioplasty of labia minora. Int J Gynaecol Obstet. 2006;93(1):38–43. https://doi.org/10.1016/j.ijgo.2006.01.002.
Placik OJ, Arkins JP. A prospective evaluation of female external genitalia sensitivity to pressure following labia Minora reduction and clitoral hood reduction. Plast Reconstr Surg. 2015;136(4):442e–52e. https://doi.org/10.1097/PRS.0000000000001573.
Alter GJ. Aesthetic labia minora and clitoral hood reduction using extended central wedge resection. Plast Reconstr Surg. 2008;122(6):1780–9. https://doi.org/10.1097/PRS.0b013e31818a9b25.
Kelishadi SS, Elston JB, Rao AJ, Tutela JP, Mizuguchi NN. Posterior wedge resection: a more aesthetic labiaplasty. Aesthet Surg J. 2013;33(6):847–53. https://doi.org/10.1177/1090820X13494755.
Rauso R, Tartaro G, Salti G, Zerbinati N, Colella G. Utilization of needles in the surgical reduction of Labia minora: A simple and cost-effective way to reduce operating time. Aesthet Surg J. 2016;36(10):NP310–2. https://doi.org/10.1093/asj/sjw159.
Choi HY, Kim KT. A new method for aesthetic reduction of labia minora (the deepithelialized reduction of labioplasty). Plast Reconstr Surg. 2000;105(1):414–9.
Cao YJ, Li FY, Li SK, et al. A modified method of labia minora reduction: the de-epithelialised reduction of the central and posterior labia minora. J Plast Reconstr Aesthet Surg. 2012;65(8):1096–102. https://doi.org/10.1016/j.bjps.2012.03.025.
Maas SM, Hage JJ. Functional and aesthetic Labia minora reduction. Plast Reconstr Surg. 2000;105(4):1453–6.
Solanki NS, Tejero-Trujeque R, Stevens-King A, Malata CM. Aesthetic and functional reduction of the labia minora using the Maas and Hage technique. J Plast Reconstr Aesthetic Surg JPRAS. 2010;63(7):1181–5. https://doi.org/10.1016/j.bjps.2009.05.053.
Gress S. Composite reduction labiaplasty. Aesthet Plast Surg. 2013;37(4):674–83. https://doi.org/10.1007/s00266-013-0149-6.
Gonzalez-Isaza P, Lotti T, Franca K, et al. Carbon dioxide with a new pulse profile and shape: A perfect tool to perform Labiaplasty for functional and cosmetic purpose. Open Access Maced J Med Sci. 2018;6(1):25–7.
Giraldo F, Gonzalez C, De Haro F. Central wedge nymphectomy with a 90-degree Z-plasty for aesthetic reduction of the labia minora. Plast Reconstr Surg. 2004;113(6):1820–5. https://doi.org/10.1097/01.PRS.0000117304.81182.96.
Kelling JA, Erickson CR, Pin J, Pin PG. Anatomical dissection of the dorsal nerve of the clitoris. Aesthet Surg J. 2020;40(5):541–7. https://doi.org/10.1093/asj/sjz330.
Jackson L, Hare A, Carrick KS, Ramirez DMO, Hammer J, Corton MM. Anatomy, Histology, and nerve density of clitoris and associated structures: clinical applications to vulvar surgery. Am J Obstet Gynecol. 2019:519.e1–9.
Tagatz G, Kopher R, Nagel T, Okagaki T. The clitoral index: a bioassay of androgenic stimulation - PubMed. Obstet Gynecol. 1979;55(5):562–4 https://pubmed.ncbi.nlm.nih.gov/503381/. Accessed 18 Sept 2020.
Wilkie G, Bartz D. Vaginal rejuvenation: A review of female genital cosmetic surgery. Obstet Gynecol Surv. 2017;73(5):287–92. https://doi.org/10.1097/OGX.0000000000000559.
Hamori CA, Banwell PE, Alinsod RM. Female Genital Cosmetic Surgery Concepts Classifications Techniques Chapter 15: O-Shot.; 2017.
Lloyd J, Crouch NS, Minto CL, Liao LM, Creighton SM. Female genital appearance: “normality” unfolds. BJOG An Int J Obstet Gynaecol. 2005;112(5):643–6. https://doi.org/10.1111/j.1471-0528.2004.00517.x.
Portman DJ, Gass MLS, Kingsberg S, et al. Genitourinary syndrome of menopause: new terminology for vulvovaginal atrophy from the international society for the study of women’s sexual health and the North American Menopause Society. Menopause. 2014;21(10):1063–8. https://doi.org/10.1097/gme.0000000000000329.
Fasola E, Gazzola R. Labia majora augmentation with hyaluronic acid filler: technique and results. Aesthet Surg J. 2016;36(10):1155–63. https://doi.org/10.1093/asj/sjw083.
Alter GJ. Management of the Mons Pubis and Labia Majora in the massive weight loss patient. Aesthet Surg J. 2009;29(5):432–42. https://doi.org/10.1016/j.asj.2009.08.015.
Krychman M, Rowan CG, Allan BB, et al. Effect of single-treatment, surface-cooled radiofrequency therapy on vaginal laxity and female sexual function: the VIVEVE I randomized controlled trial. J Sex Med. 2017;14(2):215–25. https://doi.org/10.1016/j.jsxm.2016.11.322.
Millheiser LS, Pauls RN, Herbst SJ, Chen BH. Radiofrequency Treatment of Vaginal Laxity after Vaginal Delivery: Nonsurgical Vaginal Tighteningj sm_1910 3088..3095. https://doi.org/10.1111/j.1743-6109.2010.01910.x
Sekiguchi Y, Utsugisawa Y, Azekosi Y, et al. Laxity of the vaginal introitus after childbirth: nonsurgical outpatient procedure for vaginal tissue restoration and improved sexual satisfaction using low-energy radiofrequency thermal therapy. J Women's Health. 2013;22(9):775–81. https://doi.org/10.1089/jwh.2012.4123.
Lalji S, Lozanova P. Evaluation of the safety and efficacy of a monopolar nonablative radiofrequency device for the improvement of vulvo-vaginal laxity and urinary incontinence. J Cosmet Dermatol. 2017;16(2):230–4. https://doi.org/10.1111/jocd.12348.
Fistonic I. Sorta Bilajac Turina I, Fistonic N, Marton I. short time efficacy and safety of focused monopolar radiofrequency device for labial laxity improvement - noninvasive labia tissue tightening. A prospective cohort study. Lasers Surg Med. 2016;48(3):254–9. https://doi.org/10.1002/lsm.22450.
Lordêlo P, Leal MRD, Brasil CA, Santos JM, Lima MCNPC, Sartori MGF. Radiofrequency in female external genital cosmetics and sexual function: a randomized clinical trial. Int Urogynecol J. 2016;27(11):1681–7. https://doi.org/10.1007/s00192-016-3020-x.
Jomah J, Bahi AW, Mousa KP, El-Saharty A, Neyazi SM. Treatment of vaginal relaxation syndrome with an erbium:YAG laser 360° scanning scope via automatic dual mode technique. Eur J Plast Surg. 2019;42(2):169–76. https://doi.org/10.1007/s00238-018-1472-6.
Lee MS. Treatment of vaginal relaxation syndrome with an erbium:YAG laser using 90 degrees and 360 degrees scanning scopes: A pilot Study & Short-term Results. Laser Ther. 2014;23(2):129–38. https://doi.org/10.5978/islsm.14-OR-11.
Cihantimur B, Herold C. Genital beautification: a concept that offers more than reduction of the labia minora. Aesthet Plast Surg. 2013;37(6):1128–33. https://doi.org/10.1007/s00266-013-0211-4.
de Alencar Felicio Y. Labial surgery. Aesthet Surg J. 2007;27(3):322–8. https://doi.org/10.1016/j.asj.2007.03.003.
Vogt PM, Herold C, Rennekampff HO. Autologous fat transplantation for labia majora reconstruction. Aesthet Plast Surg. 2011;35(5):913–5. https://doi.org/10.1007/s00266-011-9664-5.
Hexsel D, Dal’Forno T, Caspary P, Hexsel CL. Soft-tissue augmentation with hyaluronic acid filler for Labia majora and Mons pubis. Dermatologic Surg. 2016;42(7):911–4. https://doi.org/10.1097/DSS.0000000000000733.
El Danaf AAH. Deepithelized fasciocutaneous flap for labia majora augmentation during thigh lift. Eur J Plast Surg. 2010;33(6):373–6. https://doi.org/10.1007/s00238-010-0468-7.
Karabagli Y, Kocman EA, Velipasaoglu M, et al. Labia majora augmentation with De-epithelialized labial rim (minora) flaps as an auxiliary procedure for Labia minora reduction. Aesthet Plast Surg. 2015;39:289–93. https://doi.org/10.1007/s00266-015-0474-z.
Salgado CJ, Tang JC, Desrosiers AE III. Use of dermal fat graft for augmentation of the labia majora. J Plast Reconstr Aesthet Surg. 2012;65(2):267–70. https://doi.org/10.1016/j.bjps.2011.07.010.
Jabbour S, Kechichian E, Hersant B, et al. Labia majora augmentation: A systematic review of the literature. Aesthet Surg J. 2017;37(10):1157–64. https://doi.org/10.1093/asj/sjx056.
Goodman M, et al. Female genital plastic and cosmetic surgery. Davis: John Wiley & Sons, Ltd; 2016.
Rahman AA. Monsplasty: new technique. Plast Reconstr Surg. 2013;37(1):107–9.
Song AY, Jean RD, Hurwitz DJ, Fernstrom MH, Scott JA, Rubin JP. A classification of contour deformities after bariatric weight loss: the Pittsburgh rating scale. Plast Reconstr Surg. 2005;116(5):1535–44. https://doi.org/10.1097/01.prs.0000182606.92069.13.
El-Khatib HA. Mons pubis ptosis: classification and strategy for treatment. Aesthet Plast Surg. 2011;35(1):24–30. https://doi.org/10.1007/s00266-010-9552-4.
Marques M, Modolin M, Cintra W, Gemperli R, Ferreira MC. Monsplasty for women after massive weight loss. Aesthet Plast Surg. 2012;36(3):511–6. https://doi.org/10.1007/s00266-011-9859-9.
Bloom JMP, Van Kouwenberg E, Davenport M, Koltz PF, Shaw RBJ, Gusenoff JA. Aesthetic and functional satisfaction after monsplasty in the massive weight loss population. Aesthet Surg J. 2012;32(7):877–85. https://doi.org/10.1177/1090820X12455498.
Patoué A, De Runz A, Carloni R, Aillet S, Watier E, Bertheuil N. Safe monsplasty technique. J Plast Surg Hand Surg. 2018;52(2):74–9. https://doi.org/10.1080/2000656X.2017.1335642.
Kitzinger HB, Lumenta DB, Schrögendorfer KF, Karle B. Using superficial fascial system suspension for the management of the Mons pubis after massive weight loss. Ann Plast Surg. 2014;73(5):578–82. https://doi.org/10.1097/SAP.0b013e31827e29e5.
Alinsod RM. Transcutaneous temperature controlled radiofrequency for orgasmic dysfunction. Lasers Surg Med. 2016;48(7):641–5. https://doi.org/10.1002/lsm.22537.
Clark Z. Labial tissue rejuvenation and sexual function improvement using a novel noninvasive focused monopolar radio frequency device. J Cosmet Laser Ther. 2018;20(2):66–70. https://doi.org/10.1080/14764172.2017.1368565.
Goodman MP. Female cosmetic genital surgery. Obstet Gynecol. 2009;113(1):154–9. https://doi.org/10.1097/AOG.0b013e318190c0ea.
DeLancey JO. Anatomic aspects of vaginal eversion after hysterectomy. Am J Obstet Gynecol. 1992;166(6 Pt 1):1717–24 discussion 1724-8. http://www.ncbi.nlm.nih.gov/pubmed/1615980. Accessed 23 Mar 2018.
Hines TM. The G-spot: A modern gynecologic myth. Am J Obstet Gynecol. 2001;185(2):359–62. https://doi.org/10.1067/mob.2001.115995.
Aydın S, Sönmez FC, Karasu AFG, Gül B, Arıoğlu Ç. Search for the G spot: microvessel and nerve mapping of the paraurethral anterior vaginal wall. Int Urogynecol J. 2020;31(12):2565–72. https://doi.org/10.1007/s00192-020-04379-1.
Puppo V, Gruenwald I. Does the G-spot exist? A review of the current literature. Int Urogynecol J Pelvic Floor Dysfunct. 2012;23(12):1665–9. https://doi.org/10.1007/s00192-012-1831-y.
Haylen BT, Fischer G, Vu D, Tse K. The vaginal vestibule: assessing the case for an anterior and posterior division. Neurourol Urodyn. 2017;36(4):979–83. https://doi.org/10.1002/nau.23064.
Rogers RG, Pauls RN, Thakar R, et al. An international Urogynecological association (IUGA)/international continence society (ICS) joint report on the terminology for the assessment of sexual health of women with pelvic floor dysfunction. Neurourol Urodyn. 2018;37(4):1220–40. https://doi.org/10.1002/nau.23508.
Dietz HP, Stankiewicz M, Atan IK, Ferreira CW, Socha M. Vaginal laxity: what does this symptom mean? Int Urogynecol J. 2018;29(5):723–8. https://doi.org/10.1007/s00192-017-3426-0.
Miranne JM, Marek TM, Mete M, Iglesia CB. Prevalence and Resolution of Auditory Passage of Vaginal Air in Women With Pelvic Floor Disorders. In: Obstetrics and Gynecology. Vol 126. Lippincott Williams and Wilkins; 2015:136–143. https://doi.org/10.1097/AOG.0000000000000921.
Campbell P, Krychman M, Gray T, et al. Self-reported vaginal laxity—prevalence, impact, and associated symptoms in women attending a Urogynecology clinic. J Sex Med. 2018;15(11):1515–7. https://doi.org/10.1016/j.jsxm.2018.08.015.
Pauls RN, Fellner AN, Davila GW. Vaginal laxity: a poorly understood quality of life problem; a survey of physician members of the International Urogynecological Association (IUGA). https://doi.org/10.1007/s00192-012-1757-4
AUGS, IUGA. Joint report on terminology for surgical procedures to treat pelvic organ prolapse. Female Pelvic Med Reconstr Surg. 2020;26(3):173–201. https://doi.org/10.1097/SPV.0000000000000846.
Adamo C, Corvi M. Cosmetic mucosal vaginal tightening (Lateral Colporrhaphy): improving sexual sensitivity in women with a sensation of a wide vagina. Plast Reconstr Surg. 2009;123(6):212e–3e.
Park HJ, Jung KH, Kim SY, et al. Hyaluronic acid pulmonary embolism: a critical consequence of an illegal cosmetic vaginal procedure. Thorax. 2010;65(4):360–1. https://doi.org/10.1136/thx.2009.128272.
Yang Y, Sheng H, Gu Q, et al. Death caused by vaginal injection of hyaluronic acid and collagen: A case report. Aesthet Surg J. 2020;40(5):NP263–8. https://doi.org/10.1093/asj/sjz275.
Han SW, Park MJ, Lee SH. Hyaluronic acid-induced diffuse alveolar hemorrhage: unknown complication induced by a well-known injectable agent. Ann Transl Med. 2019;7(1):13. https://doi.org/10.21037/atm.2018.11.51.
Herold C, Motamedi M, Hartmann U, Allert S. G-spot augmentation with autologous fat transplantation. J Turkish Ger Gynecol Assoc. 2015;16(3):187–8. https://doi.org/10.5152/jtgga.2015.15027.
Runels C, Melnick H, Debourbon E, Roy L. A pilot study of the effect of localized injections of autologous platelet rich plasma (PRP) for the treatment of female sexual dysfunction. J Women’s Heal Care. 2014;3(4). https://doi.org/10.4172/2167-0420.1000169.
Evans RL, Marriott RE, Harker M. Axillary skin: biology and care. Int J Cosmet Sci. 2012;34(5):389–95. https://doi.org/10.1111/j.1468-2494.2012.00729.x.
Sharp G, Maynard P, Hamori CA, Oates J, Sarwer DB, Kulkarni J. Measuring quality of life in female genital cosmetic procedure patients: A systematic review of patient-reported outcome measures. Aesthet Surg J. 2020;40(3):311–8. https://doi.org/10.1093/asj/sjz325.
Bramwell R, Morland C. Genital appearance satisfaction in women: the development of a questionnaire and exploration of correlates. J Reprod Infant Psychol. 2009;27(1):15–27. https://doi.org/10.1080/02646830701759793.
Veale D, Eshkevari E, Ellison N, Cardozo L, Robinson D, Kavouni A. Validation of genital appearance satisfaction scale and the cosmetic procedure screening scale for women seeking labiaplasty validation of genital appearance satisfaction scale and the cosmetic procedure screening scale for women seeking labiaplasty Vali. J Psychosom Obstet Gynecol. 2013;34(1):46–52. https://doi.org/10.3109/0167482X.2012.756865.
Veale D, Naismith I, Eshkevari E, et al. Psychosexual outcome after labiaplasty: A prospective case-comparison study. Int Urogynecol J Pelvic Floor Dysfunct. 2014;25(6):831–9. https://doi.org/10.1007/s00192-013-2297-2.
Rosen R, Brown C, Heiman J, et al. The female sexual function index (Fsfi): A multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000;26(2):191–205. https://doi.org/10.1080/009262300278597.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–13. https://doi.org/10.1097/01.sla.0000133083.54934.ae.
Phillips KA, Grant J, Siniscalchi J, Albertini RS. Surgical and nonpsychiatric medical treatment of patients with body dysmorphic disorder. Psychosomatics. 2001;42(6):504–10. https://doi.org/10.1176/appi.psy.42.6.504.
Crerand CE, Menard W, Phillips KA. Surgical and minimally invasive cosmetic procedures among persons with body dysmorphic disorder. Ann Plast Surg. 2010;65(1):11–6. https://doi.org/10.1097/SAP.0b013e3181bba08f.
Sarwer DB, Wadden TA, Pertschuk MJ, Whitaker LA. Body image dissatisfaction and body dysmorphic disorder in 100 cosmetic surgery patients. Plast Reconstr Surg. 1998;101(6):1644–9. https://doi.org/10.1097/00006534-199805000-00035.
Castle DJ, Molton M, Hoffman K, Preston NJ, Phillips KA. Correlates of dysmorphic concern in people seeking cosmetic enhancement. Aust N Z J Psychiatry. 2004;38(6):439–44. https://doi.org/10.1111/j.1440-1614.2004.01381.x.
Vargel S, Ulusahin A. Psychopathology and body image in cosmetic surgery patients. Aesthet Plast Surg. 2001;25(6):474–8. https://doi.org/10.1007/s00266-001-0009-7.
Aouizerate B, Pujol H, Grabot D, et al. Body dysmorphic disorder in a sample of cosmetic surgery applicants. Eur Psychiatry. 2003;18(7):365–8. https://doi.org/10.1016/j.eurpsy.2003.02.001.
Ishigooka J, Iwao M, Suzuki M, Fukuyama Y, Murasaki M, Miura S. Demographic features of patients seeking cosmetic surgery. Psychiatry Clin Neurosci. 1998;52(3):283–7. https://doi.org/10.1046/j.1440-1819.1998.00388.x.
Vindigni V et. al. The importance of recognizing body dysmorphic disorder in cosmetic surgery patients: do our patients need a preoperative psychiatric evaluation? Eur J Plast Surg 2002;25(6):305–308.
Spriggs M, Gillam L. Body dysmorphic disorder: contraindication or ethical justification for female genital cosmetic surgery in adolescents. Bioethics. 2016;30(9):706–13. https://doi.org/10.1111/bioe.12278.
Brohede S, Wingren G, Wijma B, Wijma K. Validation of the body dysmorphic disorder questionnaire in a community sample of Swedish women. Psychiatry Res. 2013;210(2):647–52. https://doi.org/10.1016/j.psychres.2013.07.019.
Veale D, Ellison N, Werner TG, Dodhia R, Serfaty MA, Clarke A. Development of a cosmetic procedure screening questionnaire (COPS) for body dysmorphic disorder. J Plast Reconstr Aesthet Surg. 2012;65(4):530–2. https://doi.org/10.1016/j.bjps.2011.09.007.
Pauls RN, Rogers RG. Should gynecologists provide cosmetic labiaplasty procedures? AJOG. 2014;211:218–20. https://doi.org/10.1016/j.ajog.2014.06.019.
Pauls RN. Nip, tuck and rejuvenate; the latest frontier for the gynecologic surgeon. Int Urogynecol J. 2007;18(8):841–2. https://doi.org/10.1007/s00192-007-0398-5.
Iglesia CB, et al. Cosmetic Gynecology and the Elusive Quest for the “Perfect” Vagina. Obstetrics & Gynecology. 2012;119(6):1083–4. https://doi.org/10.1097/AOG.0b013e31825833f5.
World Health Organization. A Systematic Review of Health Complications of Female Genital Mutilation including Sequelae in Childbirth. 2000.
World Health Organization. Female genital mutilation. https://www.who.int/news-room/fact-sheets/detail/female-genital-mutilation. Accessed 20 Apr 2020.
ACOG CO #780. Diagnosis and Management of Hymenal Variants. Vol 133.; 2019. https://doi.org/10.1097/AOG.0000000000003283
Amy JJ. Certificates of virginity and reconstruction of the hymen. Eur J Contracept Reprod Health Care. 2008;13(2):111–3. https://doi.org/10.1080/13625180802106045.
Kandela P. Egypt’s trade in hymen repair. Lancet. 1996;347(9015):1615. https://doi.org/10.1016/s0140-6736(96)91096-x.
Raveenthiran V. Surgery of the hymen: from myth to modernisation. Indian J Surg. 2009;71(4):224–6. https://doi.org/10.1007/s12262-009-0065-9.
Paterson-Brown S. Commentary: education about the hymen is needed. BMJ. 1998;316(7129):461.
Saraiya HA. Surgical revirgination: Four vaginal mucosal flaps for reconstruction of a hymen. Indian J Plast Surg. 2015;48(2):192–5. https://doi.org/10.4103/0970-0358.163060.
Vojvodic M, Lista F, Vastis P-G, Ahmad J. Luminal reduction Hymenoplasty: A Canadian experience with hymen restoration. Aesthet Surg J. 2018;38(7):802–6. https://doi.org/10.1093/asj/sjy023.
Ou M-C, Lin C-C, Pang C-C, Ou D. A cerclage method for hymenoplasty. Taiwan J Obstet Gynecol. 2008;47(3):355–6. https://doi.org/10.1016/S1028-4559(08)60143-6.
Wei S, Li Q, Li S, Zhou C, Li F, Zhou Y. A new surgical technique of hymenoplasty. Int J Gynecol Obstet. 2015;130:14–8.
Acknowledgements
This document reflects clinical and scientific advances as of the date issued and is subject to change. The information should not be construed as dictating an exclusive course of treatment or procedure to be followed. Its content is not intended to be a substitute for professional medical judgment, diagnosis, or treatment. The ultimate judgment regarding any specific procedure or treatment is to be made by the physician and patient in light of all circumstances presented by the patient. The authors would like to thank Charlotte Holden and Marie Dauenheimer for their illustrations.
The following writing group members are being recognized for their contributions to this article: Writing Group Chair: Bobby Garcia, MD (New York City Health & Hospitals - Lincoln, Bronx, New York). IUGA Members: Rufus Cartwright, MD(res), MRCOG, PhD (Imperial College of London, UK); Samantha Conde Rocha Rangel, MD, MSC (Clinica Conde, Rio de Janeiro, Brasil); Daniela Gold, MD, PhD (Medical University Graz, Graz, Austria); Natalia Novikova, MBChB, PhD (Private Practice, Cape Town & Johannesburg, South Africa); Jennifer Jose, MD (Saint Luke’s Medical Center Global City, Taguig, Philippines). AUGS Members: Cheryl Iglesia, MD (MedStar Washington Hospital Center, Washington, DC); Linda S Burkett, MD, MSc (Magee-Womens Hospital, University of Pittsburgh Medical Center, Pittsburgh, PA); Alexis Dieter, MD (MedStar Washington Hospital Center, Washington, DC); Alexandra Dubinskaya, MD (Cedars Sinai Medical Center, Los Angeles, CA); Christine Heisler, MD (University of Wisconsin School of Medicine & Public Health, Madison, WI).
Author information
Authors and Affiliations
Consortia
Ethics declarations
Disclaimer
Inclusion of any specific procedure does not constitute an endorsement of the organizations involved in the writing of this paper, but rather an objective description for future research. We acknowledge the need for standardization of terminology within this newly emerging field with the aim of supporting and facilitating evidence-based approaches and patient care. This document aims to raise the standard on what is appropriate and acceptable while educating providers on what is commonly occurring with minimal data on safety and efficacy.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Individual writing group members are noted in the acknowledgment section.
This report is being published concurrently in Female Pelvic Medicine and Reconstructive Surgery and in International Urogynecology Journal. The report is identical except for minor stylistic and spelling differences in keeping with each journal’s style. Citations from any of the two journals can be used when citing this article.
Correspondence: Bobby Garcia, MD, New York City Health & Hospitals - Lincoln 234 East 149th Street, 5th Floor Department of OB/GYN Bronx, NY 10451, USA. E-mail: Garcia.Bobby@gmail.com
Supplementary Information
ESM 1
(DOCX 23 kb)
Rights and permissions
About this article

Cite this article
Developed by the Joint Writing Group of the International Urogynecological Association and the American Urogynecologic Society. Joint Report on Terminology for Cosmetic Gynecology. Int Urogynecol J 33, 1367–1386 (2022). https://doi.org/10.1007/s00192-021-05010-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-021-05010-7