


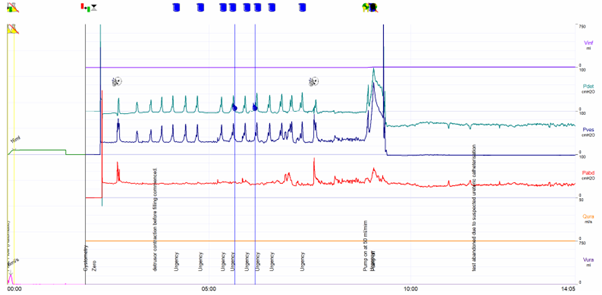
A 53-year-old female attended for urodynamic studies. She presented with symptoms of mixed urinary incontinence (urge-predominant). Her symptoms had failed to respond to anti-cholinergic and beta-3 adrenoreceptor agonist medications. As demonstrated on the trace, the patient performed a uroflowmetry test initially, which could not be reliably analyzed due to an insufficient voided volume (< 150mls). The patient underwent transurethral catheterization for the measurement of vesical pressure (blue) and vaginal catheterization for the measurement of abdominal pressure (red). The trace demonstrates that both air-filled catheters were zeroed to atmospheric pressure for reference. The catheters were ‘charged,’ whereby a small amount of air fills a micro-balloon towards the tip of the catheter, and baseline pressure measurements are recorded, with similar values displayed on both the vesical and abdominal lines. Upon asking the patient to cough to check equal pressure transmission from both the vesical and vaginal catheters, the vesical catheter was registering a higher pressure than the abdominal pressure sensor, indicated by the first spike on the detrusor line (green). The patient began to describe symptoms of urgency, yet the filling of the bladder had not commenced. There appear to be phasic increases in vesical pressure, which correspond with the patient’s symptoms of urgency. This is reflected on the detrusor line as sharp, regular increases in detrusor pressure, which appear uniform and within quick succession of one another. Upon attempting to fill the bladder, the patient experienced extreme pain, and there was a significant rise in vesical pressure. The patient experienced sweating, dizziness, and nausea. The catheters were removed immediately. The trace demonstrates ureteric catheterization, which displays uniform, peristaltic-like increases in vesical pressure and a greater, sudden increase in vesical pressure upon filling of the bladder. A diagnosis of phasic detrusor overactivity could have mistakenly been made; however, the vesical pressure increases are sharp in nature, uniform, and regular, which indicates ureteric peristalsis. This corresponds with the patient’s symptoms of pain, dizziness, and nausea.